
Page 800 - Clinical Immunology_ Principles and Practice ( PDFDrive )
P. 800
CHaPtEr 57 Spondyloarthritis 771
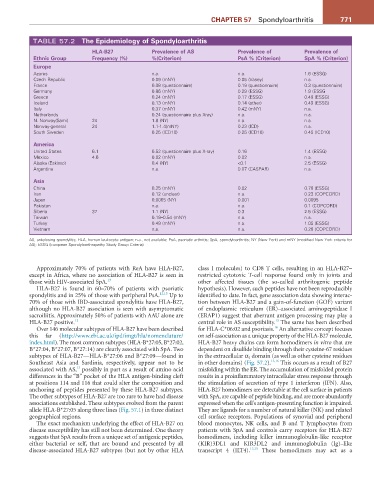
TABLE 57.2 the Epidemiology of spondyloarthritis
HLa-B27 Prevalence of as Prevalence of Prevalence of
Ethnic Group Frequency (%) %(Criterion) Psa % (Criterion) spa % (Criterion)
Europe
Azores n.a. n.a. 1.6 (ESSG)
Czech Republic 0.09 (mNY) 0.05 (Vasey) n.a.
France 0.08 (questionnaire) 0.19 (questionnaire) 0.3 (questionnaire)
Germany 0.86 (mNY) 0.29 (ESSG) 1.9 (ESSG
Greece 0.24 (mNY) 0.17 (ESSG) 0.49 (ESSG)
Iceland 0.13 (mNY) 0.14 (other) 0.49 (ESSG)
Italy 0.37 (mNY) 0.42 (mNY) n.a.
Netherlands 0.24 (questionnaire plus Xray) n.a. n.a.
N. Norway(Sami) 24 1.8 (NY) n.a. n.a.
Norway-general 24 1.1-1.4(mNY) 0.23 (ICD) n.a.
South Sweden 0.25 (ICD10) 0.25 (ICD10) 0.45 (ICD10)
america
United States 6.1 0.52 (questionnaire plus X-ray) 0.16 1.4 (ESSG)
Mexico 4.6 0.02 (mNY) 0.02 n.a.
Alaska (Eskimo) 0.4 (NY) <0.1 2.5 (ESSG)
Argentina n.a. 0.07 (CASPAR) n.a.
asia
China 0.25 (mNY) 0.02 0.78 (ESSG)
Iran 0.12 (unclear) n.a. 0.23 (COPCORD)
Japan 0.0065 (NY) 0.001 0.0095
Pakistan n.a. n.a. 0.1 (COPCORD)
Siberia 37 1.1 (NY) 0.3 2.5 (ESSG)
Taiwan 0.19–0.54 (mNY) n.a. n.a.
Turkey 0.49 (mNY) n.a. 1.05 (ESSG)
Vietnam n.a. n.a. 0.28 (COPCORD)
AS, ankylosing spondylitis; HLA, human leukocyte antigen; n.a., not available; PsA, psoriatic arthritis; SpA, spondyloarthritis; NY (New York) and mNY (modified New York criteria for
AS); ESSG (European Spondyloarthropathy Study Group Criteria)
Approximately 70% of patients with ReA have HLA-B27, class I molecules) to CD8 T cells, resulting in an HLA-B27–
except in Africa, where no association of HLA-B27 is seen in restricted cytotoxic T-cell response found only in joints and
those with HIV-associated SpA. 13 other affected tissues (the so-called arthritogenic peptide
HLA-B27 is found in 60–70% of patients with psoriatic hypothesis). However, such peptides have not been reproducibly
spondylitis and in 25% of those with peripheral PsA. 12,13 Up to identified to date. In fact, gene association data showing interac-
70% of those with IBD-associated spondylitis have HLA-B27, tion between HLA-B27 and a gain-of-function (GOF) variant
although no HLA-B27 association is seen with asymptomatic of endoplasmic reticulum (ER)–associated aminopeptidase I
sacroiliitis. Approximately 50% of patients with AAU alone are (ERAP1) suggest that aberrant antigen processing may play a
15
HLA-B27 positive. 12 central role in AS susceptibility. The same has been described
16
Over 146 molecular subtypes of HLA-B27 have been described for HLA-C*06:02 and psoriasis. An alternative concept focuses
this far (http://www.ebi.ac.uk/ipd/imgt/hla/nomenclature/ on self-association as a unique property of the HLA-B27 molecule.
index.html). The most common subtypes (HLA-B*27:05, B*27:02, HLA-B27 heavy chains can form homodimers in vitro that are
B*27:04, B*27:07, B*27:14) are clearly associated with SpA. Two dependent on disulfide binding through their cysteine-67 residues
subtypes of HLA-B27—HLA-B*27:06 and B*27:09—found in in the extracellular α 1 domain (as well as other cysteine residues
Southeast Asia and Sardinia, respectively, appear not to be in other domains) (Fig. 57.2). 13,16 This occurs as a result of B27
13
associated with AS, possibly in part as a result of amino acid misfolding within the ER. The accumulation of misfolded protein
differences in the “B” pocket of the HLA antigen-binding cleft results in a proinflammatory intracellular stress response through
at positions 114 and 116 that could alter the composition and the stimulation of secretion of type 1 interferon (IFN). Also,
anchoring of peptides presented by these HLA-B27 subtypes. HLA-B27 homodimers are detectable at the cell surface in patients
The other subtypes of HLA-B27 are too rare to have had disease with SpA, are capable of peptide binding, and are more abundantly
associations established. These subtypes evolved from the parent expressed when the cell’s antigen-presenting function is impaired.
allele HLA-B*27:05 along three lines (Fig. 57.1) in three distinct They are ligands for a number of natural killer (NK) and related
geographical regions. cell surface receptors. Populations of synovial and peripheral
The exact mechanism underlying the effect of HLA-B27 on blood monocytes, NK cells, and B and T lymphocytes from
disease susceptibility has still not been determined. One theory patients with SpA and controls carry receptors for HLA-B27
suggests that SpA results from a unique set of antigenic peptides, homodimers, including killer immunoglobulin-like receptor
either bacterial or self, that are bound and presented by all (KIR)3DL1 and KIR3DL2 and immunoglobulin (Ig)–like
disease-associated HLA-B27 subtypes (but not by other HLA transcript 4 (ILT4). 13,15 These homodimers may act as a