
Page 822 - Clinical Immunology_ Principles and Practice ( PDFDrive )
P. 822
794 Part SIX Systemic Immune Diseases
$FWLYDWHG 301 $FWLYDWHG 301
5HVWLQJ 301 5HVWLQJ 301
,QWUDYDVFXODU ,QWUDYDVFXODU
VSDFH VSDFH
([WUDYDVFXODU ([WUDYDVFXODU
VSDFH VSDFH
$ %
$FWLYDWHG 301 $FWLYDWHG 301
5HVWLQJ 301 5HVWLQJ 301
5HFUXLWPHQW
,QWUDYDVFXODU ,QWUDYDVFXODU
VSDFH VSDFH
([WUDYDVFXODU ([WUDYDVFXODU
VSDFH VSDFH
$FXWH LQIODPPDWLRQ &KURQLF
& ' ZLWK 1(7 IRUPDWLRQ LQIODPPDWLRQ
(QGRWKHOLDO FHOO &RPSOHPHQW *$ )LEUREODVW 7 FHOO
UHFHSWRU DQG & H
$QWLQHXWURSKLO
5HVWLQJ DQG F\WRSODVPLF DQWLERG\
DFWLYDWHG QHXWURSKLO $1&$ 0RQRF\WH DQG &' E
SRO\PRUSKRQXFOHDU FHOO 301 DQG SURWHLQDVH FU PDFURSKDJH
P\HORSURWHLQDVH
&\WRNLQH UHFHSWRU ,QWUDFHOOXODU DGKHVLRQ
DQG SURLQIODPPDWRU\ PROHFXOH ,&$0 )F UHFHSWRU )LEULQ &ROODJHQ
F\WRNLQH
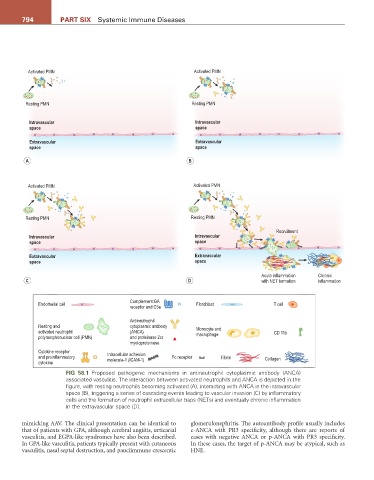
FIG 58.1 Proposed pathogenic mechanisms in antineutrophil cytoplasmic antibody (ANCA)
associated vasculitis. The interaction between activated neutrophils and ANCA is depicted in the
figure, with resting neutrophils becoming activated (A), interacting with ANCA in the intravascular
space (B), triggering a series of cascading events leading to vascular invasion (C) by inflammatory
cells and the formation of neutrophil extracellular traps (NETs) and eventually chronic inflammation
in the extravascular space (D).
mimicking AAV. The clinical presentation can be identical to glomerulonephritis. The autoantibody profile usually includes
that of patients with GPA, although cerebral angiitis, urticarial c-ANCA with PR3 specificity, although there are reports of
vasculitis, and EGPA-like syndromes have also been described. cases with negative ANCA or p-ANCA with PR3 specificity.
In GPA-like vasculitis, patients typically present with cutaneous In these cases, the target of p-ANCA may be atypical, such as
vasculitis, nasal septal destruction, and pauciimmune crescentic HNE.