
Page 1199 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1199
836 PART 6: Neurologic Disorders
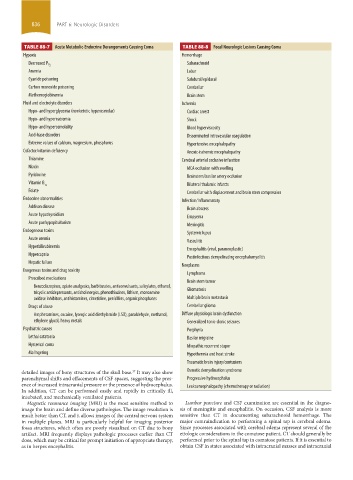
TABLE 88-7 Acute Metabolic-Endocrine Derangements Causing Coma TABLE 88-8 Focal Neurologic lesions Causing Coma
Hypoxia Hemorrhage
Subarachnoid
Decreased P O 2
Anemia Lobar
Cyanide poisoning Subdural/epidural
Carbon monoxide poisoning Cerebellar
Methemoglobinemia Brain stem
Fluid and electrolyte disorders Ischemia
Hypo- and hyperglycemia (nonketotic hyperosmolar) Cardiac arrest
Hypo- and hypernatremia Shock
Hypo- and hyperosmolality Blood hyperviscosity
Acid-base disorders Disseminated intravascular coagulation
Extreme values of calcium, magnesium, phosphorus Hypertensive encephalopathy
Cofactor/vitamin deficiency Anoxic-ischemic encephalopathy
Thiamine Cerebral arterial occlusive infarction
Niacin MCA occlusion with swelling
Pyridoxine Brainstem/basilar artery occlusion
Vitamin B
12 Bilateral thalamic infarcts
Folate Cerebellar with displacement and brain stem compression
Endocrine abnormalities Infection/Inflammatory
Addison disease Brain abscess
Acute hypothyroidism Empyema
Acute panhypopituitarism Meningitis
Endogenous toxins Systemic lupus
Acute uremia Vasculitis
Hyperbilirubinemia
Encephalitis (viral, paraneoplastic)
Hypercapnia
Postinfectious demyelinating encephalomyelitis
Hepatic failure
Neoplasms
Exogenous toxins and drug toxicity
Lymphoma
Prescribed medications Brain stem tumor
Benzodiazepines, opiate analgesics, barbiturates, anticonvulsants, salicylates, ethanol,
tricyclic antidepressants, anticholinergics, phenothiazines, lithium, monoamine Gliomatosis
oxidase inhibitors, antihistamines, cimetidine, penicillins, organic phosphates Multiple brain metastasis
Drugs of abuse Cerebellar glioma
Amphetamines, cocaine, lysergic acid diethylamide (LSD), paraldehyde, methanol, Diffuse physiologic brain dysfunction
ethylene glycol, heavy metals Generalized tonic-clonic seizures
Psychiatric causes Porphyria
Lethal catatonia Basilar migraine
Hysterical coma Idiopathic recurrent stupor
Malingering Hypothermia and heat stroke
Traumatic brain injury/contusions
detailed images of bony structures of the skull base. It may also show Osmotic demyelination syndrome
37
parenchymal shifts and effacements of CSF spaces, suggesting the pres- Progressive hydrocephalus
ence of increased intracranial pressure or the presence of hydrocephalus. Leukoencephalopathy (chemotherapy or radiation)
In addition, CT can be performed easily and rapidly in critically ill,
intubated, and mechanically ventilated patients.
Magnetic resonance imaging (MRI) is the most sensitive method to Lumbar puncture and CSF examination are essential in the diagno-
image the brain and define diverse pathologies. The image resolution is sis of meningitis and encephalitis. On occasion, CSF analysis is more
much better than CT, and it allows images of the central nervous system sensitive than CT in documenting subarachnoid hemorrhage. The
in multiple planes. MRI is particularly helpful for imaging posterior major contraindication to performing a spinal tap is cerebral edema.
fossa structures, which often are poorly visualized on CT due to bony Since processes associated with cerebral edema represent several of the
artifact. MRI frequently displays pathologic processes earlier than CT etiologic considerations in the comatose patient, CT should generally be
does, which may be critical for prompt initiation of appropriate therapy, performed prior to the spinal tap in comatose patients. If it is essential to
as in herpes encephalitis. obtain CSF in states associated with intracranial masses and intracranial
section06.indd 836 1/23/2015 12:56:24 PM