
Page 1196 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1196
CHAPTER 88: Coma, Persistent Vegetative State, and Brain Death 833
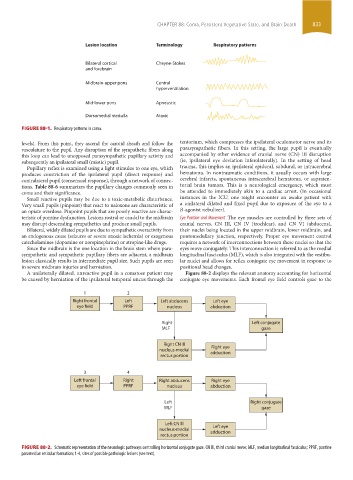
Lesion location Terminology Respiratory patterns
Bilateral cortical Cheyne-Stokes
and forebrain
Midbrain-upper pons Central
hyperventilation
Mid-lower pons Apneustic
Dorsomedial medulla Ataxic
FIGURE 88-1. Respiratory patterns in coma.
levels). From this point, they ascend the carotid sheath and follow the tentorium, which compresses the ipsilateral oculomotor nerve and its
vasculature to the pupil. Any disruption of the sympathetic fibers along parasympathetic fibers. In this setting, the large pupil is eventually
this loop can lead to unopposed parasympathetic pupillary activity and accompanied by other evidence of cranial nerve (CN) III disruption
subsequently an ipsilateral small (miotic) pupil. (ie, ipsilateral eye deviation inferolaterally). In the setting of head
Pupillary reflex is examined using a light stimulus to one eye, which trauma, this implies an ipsilateral epidural, subdural, or intracerebral
produces constriction of the ipsilateral pupil (direct response) and hematoma. In nontraumatic conditions, it usually occurs with large
contralateral pupil (consensual response), through a network of connec- cerebral infarcts, spontaneous intracerebral hematoma, or supraten-
tions. Table 88-6 summarizes the pupillary changes commonly seen in torial brain tumors. This is a neurological emergency, which must
coma and their significance. be attended to immediately akin to a cardiac arrest. (In occasional
Small reactive pupils may be due to a toxic-metabolic disturbance. instances in the ICU, one might encounter an awake patient with
Very small pupils (pinpoint) that react to naloxone are characteristic of a unilateral dilated and fixed pupil due to exposure of the eye to a
an opiate overdose. Pinpoint pupils that are poorly reactive are charac- β-agonist nebulizer).
teristic of pontine dysfunction. Lesions rostral or caudal to the midbrain Eye Position and Movement The eye muscles are controlled by three sets of
may disrupt descending sympathetics and produce small pupils. cranial nerves, CN III, CN IV (trochlear), and CN VI (abducens),
Bilateral, widely dilated pupils are due to sympathetic overactivity from their nuclei being located in the upper midbrain, lower midbrain, and
an endogenous cause (seizures or severe anoxic ischemia) or exogenous pontomedullary junction, respectively. Proper eye movement control
catecholamines (dopamine or norepinephrine) or atropine-like drugs. requires a network of interconnections between these nuclei so that the
Since the midbrain is the one location in the brain stem where para- eyes move conjugately. This interconnection is referred to as the medial
sympathetic and sympathetic pupillary fibers are adjacent, a midbrain longitudinal fasciculus (MLF), which is also integrated with the vestibu-
lesion classically results in intermediate pupil size. Such pupils are seen lar nuclei and allows for reflex conjugate eye movement in response to
in severe midbrain injuries and herniation. positional head changes.
A unilaterally dilated, unreactive pupil in a comatose patient may Figure 88-2 displays the relevant anatomy accounting for horizontal
be caused by herniation of the ipsilateral temporal uncus through the conjugate eye movements. Each frontal eye field controls gaze to the
1 2
Right frontal Left Left abducens Left eye
eye field PPRF nucleus abduction
Right Left conjugate
MLF gaze
Right CN lll
Right eye
nucleus-medial adduction
rectus portion
3 4
Left frontal Right Right abducens Right eye
eye field PPRF nucleus abduction
Left Right conjugate
MLF gaze
Left CN lll
Left eye
nucleus-medial adduction
rectus portion
FIGURE 88-2. Schematic representation of the neurologic pathways controlling horizontal conjugate gaze. CN III, third cranial nerve; MLF, median longitudinal fasciculus; PPRF, pontine
paramedian reticular formation; 1-4, sites of possible pathologic lesions (see text).
section06.indd 833 1/23/2015 12:56:22 PM