
Page 1472 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1472
CHAPTER 105: Gastrointestinal Hemorrhage 1011
TABLE 105-3 Child-Pugh Classification of Hepatic Disease Severity should be the vasoactive agent of choice. Agents that have β -agonist
2
activity, such as dopamine, should be avoided because they potentially
Points Assigned could cause splanchnic vasodilation and therefore worsen the variceal
Parameter 1 2 3 bleed. Splanchnic vasoconstrictors such as octreotide and terlipressin
(discussed later) can have a beneficial effect on systemic blood pressure
Ascites Absent Slight Moderate
by diverting blood away from the splanchnic circulation. Endotracheal
Bilirubin (mg/dL) <2 2-3 >3 intubation for airway protection is critical, especially in the setting of
Albumin (g/dL) >3.5 2.8-3.5 <2.8 encephalopathy, active hematemesis, or emergent endoscopy.
INR <1.7 1.8-2.3 >2.3 Infection: Cirrhosis is characterized by cellular and humoral immune
Encephalopathy None Grade 1-2 Grade 3-4 dysfunction, and increased bacterial translocation from the gut into
the bloodstream, facilitating the development of infections. The most
Total Score (Five Parameters) Child-Pugh Stage common bacterial infections are caused by gram-negative bacteria, pro-
5-6 A ducing spontaneous bacterial peritonitis (25%), urinary tract infections
(20%), pneumonia (15%), and bacteremia (12%). 29,30 The presence of
7-9 B
infection has been associated with failure to control the initial bleed and
10-15 C an increase in the recurrence of rebleeding, likely owing to the induc-
tion of a hyperdynamic circulation and increased portal pressure. 31,32
hemorrhage in the setting of cirrhosis predisposes the patient to specific A recent meta-analysis and systematic review of studies regarding the
derangements, including hepatic encephalopathy, type 1 hepatorenal use of prophylactic antibiotics in cirrhotics with upper gastrointestinal
syndrome, and systemic infection. These processes contribute to the bleeding concluded that antibiotics reduced bacterial infections, all-
high mortality associated with variceal bleeding, and therefore, the man- cause mortality, bacterial infection–related mortality, rebleeding events,
29
agement should address these issues in addition to achieving hemostasis and hospitalization length ; therefore, the administration of antibiot-
and hemodynamic stability. ics in the setting of variceal bleeding has become the standard of care.
Although most of the pertinent studies include a quinolone, the optimal
Cardiopulmonary: Fluid resuscitation should be aimed at achieving choice and duration of antibiotic therapy have not been defined, and
a euvolemic status because this approach prevents persistent portal therefore, the choice of empiric antibiotic therapy should be institution
hypertension and recurrent variceal bleeding. To this end, invasive specific. One study from Spain showed that intravenous ceftriaxone is
28
hemodynamic monitoring with a central venous catheter can be used more effective than oral norfloxacin ; however, this was likely second-
33
to guide fluid therapy. In the setting of hypotension that is refractory to ary to high incidence of quinolone resistance in that patient population.
fluid resuscitation, a peripheral vasoconstrictor such as norepinephrine The choice of nonfluoroquinolone antibiotic therapy is an important
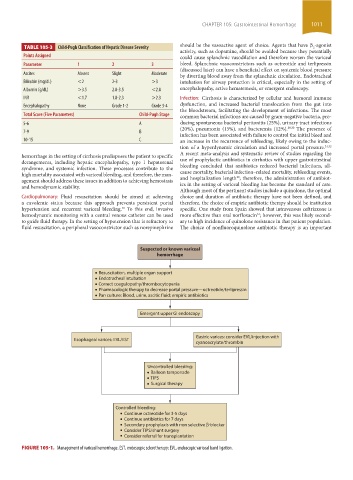
Suspected or known variceal
hemorrhage
• Resuscitation, multiple organ support
• Endotracheal intubation
• Correct coagulopathy/thrombocytopenia
• Pharmacologic therapy to decrease portal pressure—octreotide/terlipressin
• Pan culture: Blood, urine, ascitic fluid; empiric antibiotics
Emergent upper GI endoscopy
Gastric varices: consider EVL/injection with
Esophageal varices: EVL/EST
cyanoacrylate/thrombin
Uncontrolled bleeding:
• Balloon tamponade
• TIPS
• Surgical therapy
Controlled bleeding:
Continue octreotide for 3-5 days
Continue antibiotics for 7 days
Secondary prophylaxis with non selective -blocker
Consider TIPS/shunt surgery
Consider referral for transplantation
FIGURE 105-1. Management of variceal hemorrhage. EST, endoscopic sclerotherapy; EVL, endoscopic variceal band ligation.
section09.indd 1011 1/19/2015 10:54:27 PM