
Page 1555 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1555
1074 PART 10: The Surgical Patient
FIGURE 112-3. Radiographic findings of cardiac herniation. A. Herniation to the left pleural cavity; inferiorly displaced cardiac silhouette. B. Herniation to the right pleural cavity; rightward
displacement of cardiac silhouette.
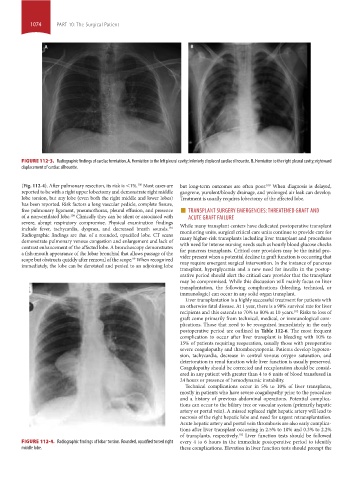
(Fig. 112-4). After pulmonary resection, its risk is <1%. Most cases are but long-term outcomes are often poor. When diagnosis is delayed,
100
100
reported to be with a right upper lobectomy and demonstrate right middle gangrene, purulent/bloody drainage, and prolonged air leak can develop.
lobe torsion, but any lobe (even both the right middle and lower lobes) Treatment is usually requires lobectomy of the affected lobe.
has been reported. Risk factors a long vascular pedicle, complete fissure,
free pulmonary ligament, pneumothorax, pleural effusion, and presence ■ TRANSPLANT SURGERY EMERGENCIES: THREATENED GRAFT AND
of a nonventilated lobe. Clinically they can be silent or associated with ACUTE GRAFT FAILURE
100
severe, abrupt respiratory compromise. Physical examination findings
include fever, tachycardia, dyspnea, and decreased breath sounds. While many transplant centers have dedicated postoperative transplant
101
monitoring units, surgical critical care units continue to provide care for
Radiographic findings are that of a rounded, opacified lobe. CT scans
demonstrate pulmonary venous congestion and enlargement and lack of many higher-risk transplants including liver transplant and procedures
with need for intense nursing needs such as hourly blood glucose checks
contrast enhancement of the affected lobe. A bronchoscopy demonstrates
a fish-mouth appearance of the lobar bronchial that allows passage of the for pancreas transplants. Critical care providers may be the initial pro-
vider present when a potential decline in graft function is occurring that
scope but obstructs quickly after removal of the scope. When recognized
99
immediately, the lobe can be derotated and pexied to an adjoining lobe may require emergent surgical intervention. In the instance of pancreas
transplant, hyperglycemia and a new need for insulin in the postop-
erative period should alert the critical care provider that the transplant
may be compromised. While this discussion will mainly focus on liver
transplantation, the following complications (bleeding, technical, or
immunologic) can occur in any solid organ transplant.
Liver transplantation is a highly successful treatment for patients with
an otherwise fatal disease. At 1 year, there is a 90% survival rate for liver
recipients and this extends to 70% to 80% at 10 years. Risks to loss of
102
graft come primarily from technical, medical, or immunological com-
plications. Those that need to be recognized immediately in the early
postoperative period are outlined in Table 112-6. The most frequent
complication to occur after liver transplant is bleeding with 10% to
15% of patients requiring reoperation, usually those with preoperative
severe coagulopathy and thrombocytopenia. Patients develop hypoten-
sion, tachycardia, decrease in central venous oxygen saturation, and
deterioration in renal function while liver function is usually preserved.
Coagulopathy should be corrected and reexploration should be consid-
ered in any patient with greater than 4 to 6 units of blood transfused in
24 hours or presence of hemodynamic instability.
Technical complications occur in 5% to 10% of liver transplants,
mostly in patients who have severe coagulopathy prior to the procedure
and a history of previous abdominal operations. Potential complica-
tions can occur to the biliary tree or vascular system (primarily hepatic
artery or portal vein). A missed replaced right hepatic artery will lead to
necrosis of the right hepatic lobe and need for urgent retransplantation.
Acute hepatic artery and portal vein thrombosis are also early complica-
tions after liver transplant occurring in 2.5% to 10% and 0.3% to 2.2%
of transplants, respectively. Liver function tests should be followed
102
FIGURE 112-4. Radiographic findings of lobar torsion. Rounded, opacified torsed right every 4 to 6 hours in the immediate postoperative period to identify
middle lobe. these complications. Elevation in liver function tests should prompt the
section10.indd 1074 1/20/2015 9:19:46 AM