
Page 1567 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1567
1086 PART 10: The Surgical Patient
https://kat.cr/user/tahir99/
30
20
10
0
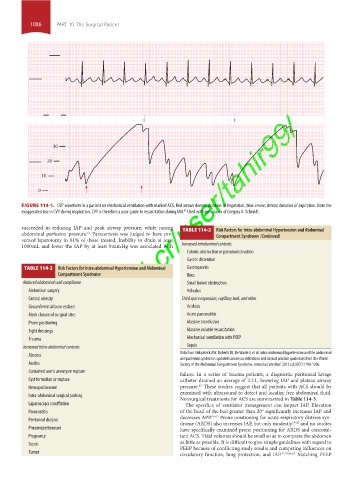
FIGURE 114-1. CVP waveform in a patient on mechanical ventilation with marked ACS. Red arrows denote duration of inspiration, blue arrows denote duration of expiration. Note the
47
exaggerated rise in CVP during inspiration. CVP is therefore a poor guide to resuscitation during IAH. Used with permission of Gregory A. Schmidt.
succeeded in reducing IAP and peak airway pressure, while raising TABLE 114-2 Risk Factors for intra-abdominal Hypertension and Abdominal
abdominal perfusion pressure. Paracentesis was judged to have pre- Compartment Syndrome (Continued)
61
vented laparotomy in 81% of those treated. Inability to drain at least
1000 mL and lower the IAP by at least 9 mm Hg was associated with Increased intraluminal contents
Colonic obstruction or pseudoobstruction
Gastric distention
TABLE 114-2 Risk Factors for intra-abdominal Hypertension and Abdominal Gastroparesis
Compartment Syndrome Ileus
Reduced abdominal wall compliance Small bowel obstruction
Abdominal surgery Volvulus
Central obesity Third space expansion, capillary leak, and other
Circumferential burn eschars Acidosis
Mesh closure of surgical sites Acute pancreatitis
Prone positioning Massive transfusion
Tight dressings Massive volume resuscitation
Trauma Mechanical ventilation with PEEP
Increased intra-abdominal contents Sepsis
Data from Kirkpatrick AW, Roberts DJ, De Waele J, et al. Intra-abdominal hypertension and the abdominal
Abscess
compartment syndrome: updated consensus definitions and clinical practice guidelines from the World
Ascites Society of the Abdominal Compartment Syndrome. Intensive Care Med. 2013 Jul;39(7):1190-1206.
Contained aortic aneurysm rupture
failure. In a series of trauma patients, a diagnostic peritoneal lavage
Cyst formation or rupture catheter drained an average of 2.2 L, lowering IAP and plateau airway
62
Hemoperitoneum pressure. These studies suggest that all patients with ACS should be
examined with ultrasound to detect and localize free abdominal fluid.
Intra-abdominal surgical packing
Nonsurgical treatments for ACS are summarized in Table 114-3.
Laparoscopic insufflation The specifics of ventilator management can impact IAP. Elevation
Pancreatitis of the head of the bed greater than 20° significantly increases IAP and
decreases APP. 63-65 Prone positioning for acute respiratory distress syn-
Peritoneal dialysis drome (ARDS) also increases IAP, but only modestly 18-20 and no studies
Pneumoperitoneum have specifically examined prone positioning for ARDS and concomi-
Pregnancy tant ACS. Tidal volumes should be small so as to compress the abdomen
Sepsis as little as possible. It is difficult to give simple guidelines with regard to
PEEP because of conflicting study results and competing influences on
Tumor circulatory function, lung protection, and IAP. 21,22,66,67 Matching PEEP
section10.indd 1086 1/20/2015 9:19:51 AM