
Page 1850 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1850
CHAPTER 132: Diving Medicine and Drowning 1319
. Continuing CO 2 to distinguish it from unconsciousness after breath-hold swimming
as the alveolar P CO 2 approaches the mixed venous P CO 2
, which then allows the alve- events performed entirely in shallow water, such as in pools. Both types
3
production increases the mixed venous P CO 2
causes breathing to resume of events are responsible for many episodes of drowning.
olar P CO 2 to increase further. The rising P CO 2
at the so-called break point. The time to the break point can be extended In breath-hold diving, the physiology is modified by a diving response
such as hyperventila- induced by apnea and facial immersion, particularly if the water is cold.
by maneuvers that lower the P CO 2 or raise the P O 2
tion or O 2 breathing. Hyperventilation does not appreciably increase the This diving response, manifested by the triad of apnea, bradycardia,
resulting from a and redistribution of organ blood flow is most pronounced in young
body’s O 2 stores because the increase in alveolar P O 2
only increases blood O 2 content slightly. Thus, children. It has been interpreted as an O 2-conserving response that
decrease in alveolar P CO 2
hyperventilation extends breath-hold time, but profound hypoxia may redistributes blood flow from organs resistant to hypoxia to organs with
develop before the CO 2 reaches the break point. continuous O 2 needs such as heart and brain. This diving response may
The physiology of breath-holding is altered by underwater descent convey a small advantage to trained human apnea divers, and it probably
because the thoracic compression decreases the lung volume, which does contribute to the survival of children after submersion in cold water.
increases the partial pressures of O 2, CO 2, and N 2 in the lungs (Fig. 132-1).
The alveolar O 2 and CO 2 concentrations decrease faster than the inert DIVING WITH COMPRESSED GASES
gas (N 2) because those gases are transferred more quickly to the pulmo-
nary capillary blood as O is consumed and since CO 2 is more soluble The practical utility of underwater breath-hold diving is limited by time
2
than nitrogen. and depth, although today there are still working free divers, such as the
initially Japanese Ama, and competitive, “no-limit” apnea divers have achieved
Compared with a simple breath-hold in air, the alveolar P O 2
increases during a breath-hold dive due to the increase in pressure on depths exceeding 200 m. The use of pressurized underwater breathing
the thorax. The transfer of CO 2 during the early descent is opposite apparatus provides the diver with a continuous supply of breathing gas
normal, and CO 2 moves from alveoli to pulmonary capillary blood. at almost any depth. In shallow water, for instance, 0 to 135 fsw, diving
During ascent, the lung re-expands, and as the pressure decreases, so is usually carried out with compressed air because it is inexpensive
may and readily available, even at remote locations. Air divers are usually
do the alveolar P O 2 and P CO 2 . Near the surface, the alveolar P O 2
, and during ascent from particularly free swimming, that is, they use a self-contained underwater breathing
approach the mixed venous P O 2
strenuous dives, the expansion of hypoxic alveoli may result in reverse apparatus (SCUBA). Special gas mixtures, such as 32% nitrogen-oxygen
O 2 transfer from mixed venous blood to alveoli (see Fig. 132-1). Carbon (nitrox), used to extend the bottom time and/or provide an extra safety
dioxide in the blood during the dive also leaves during ascent as alveolar margin, are increasingly being used by recreational divers.
decreases. Carbon dioxide elimination continues after the dive as The recommended maximum safe depth for Scuba divers is 135 fsw
P CO 2
does the elimination of the small amount of N 2 that entered the blood and approximately 200 fsw for divers tethered to a safety line. Safety
4
during the dive. concerns are brought about by three factors: nitrogen narcosis, safe
Hyperventilation before a breath-hold dive is a dangerous way to decompression, and oxygen toxicity. The problems of importance to
initially increases the intensive care specialist are related to decompression illness and
extend the duration of dive. Because the alveolar P O 2
from thoracic compression, the primary signal to return to the surface is pulmonary overpressurization as discussed below. The other problems
. If the diver hyperventilates before the breath-hold, the arterial are covered in standard textbooks on diving medicine.
the P CO 2
begins at a lower level, which extends the time to the break point. To dive beyond the practical range of compressed air, special gas mix-
P CO 2
During the longer dive, the alveolar O 2 concentration decreases to lower tures, such as helium-oxygen (heliox) or oxygen-enriched air (nitrox)
levels, and as the diver approaches the surface, life-threatening hypoxia must be supplied. In heliox operations, inspired oxygen pressure is
and loss of consciousness may occur. Traditionally, this is called shallow usually maintained at a constant 0.4 to 1.0 ATA, and the helium may
water blackout, although free divers may refer to it as deep water blackout be recycled by gas reconditioning equipment. Surface-supplied heliox
A D
Pa Pa Pa Pa
Pv O 2 CO 2 Pa Pv O 2 CO 2 Pa
O 2 120 25 O 2 O 2 30 45 O 2
40 110 35 30
Pv Pa Pv Pa
CO 2 CO 2 CO 2 CO 2
46 25 55 45
Descent Ascent
B C
Pv O 2 150 25 Pa O 2 Pv O 2 35 50 Pa O 2
40 135 Breath-hold time 35 35
Pv Pa Pv Pa
CO 2 CO 2 CO 2 CO 2
46 30 55 50
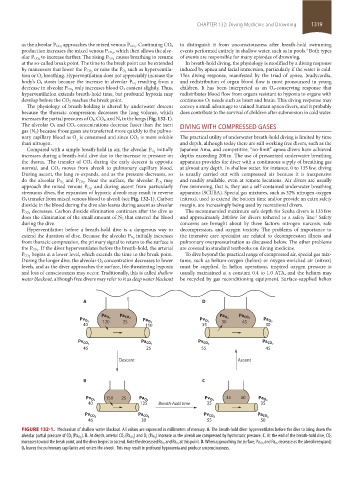
FIGURE 132-1. Mechanism of shallow water blackout. All values are expressed in millimeters of mercury. A. The breath-hold diver hyperventilates before the dive to bring down the
) increase as the alveoli are compressed by hydrostatic pressure. C. At the end of the breath-hold dive, CO 2
alveolar partial pressure of CO 2 (Pa CO 2 ). B. At depth, arterial CO 2 (Pa CO 2 ) and O 2 (Pa O 2
decrease as the alveoli reexpand;
increases toward the break point, and the diver begins to ascend. Note the decreased Pa O 2 and Pa O 2 at this point. D. When approaching the surface, Pa CO 2 and Pa O 2
O 2 leaves the pulmonary capillaries and enters the alveoli. This may result in profound hypoxemia and produce unconsciousness.
section11.indd 1319 1/19/2015 10:56:09 AM