
Page 126 - Clinical Anatomy
P. 126
ECA2 7/18/06 6:43 PM Page 111
The urinary tract 111
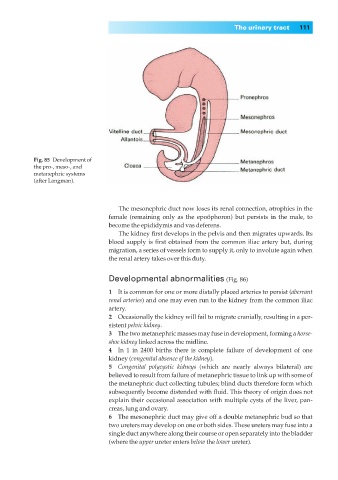
Fig. 85◊Development of
the pro-, meso-, and
metanephric systems
(after Langman).
The mesonephric duct now loses its renal connection, atrophies in the
female (remaining only as the epoöphoron) but persists in the male, to
become the epididymis and vas deferens.
The kidney first develops in the pelvis and then migrates upwards. Its
blood supply is first obtained from the common iliac artery but, during
migration, a series of vessels form to supply it, only to involute again when
the renal artery takes over this duty.
Developmental abnormalities (Fig. 86)
1◊◊It is common for one or more distally placed arteries to persist (aberrant
renal arteries) and one may even run to the kidney from the common iliac
artery.
2◊◊Occasionally the kidney will fail to migrate cranially, resulting in a per-
sistent pelvic kidney.
3◊◊The two metanephric masses may fuse in development, forming a horse-
shoe kidney linked across the midline.
4◊◊In 1 in 2400 births there is complete failure of development of one
kidney (congenital absence of the kidney).
5◊◊Congenital polycystic kidneys (which are nearly always bilateral) are
believed to result from failure of metanephric tissue to link up with some of
the metanephric duct collecting tubules; blind ducts therefore form which
subsequently become distended with fluid. This theory of origin does not
explain their occasional association with multiple cysts of the liver, pan-
creas, lung and ovary.
6◊◊The mesonephric duct may give off a double metanephric bud so that
two ureters may develop on one or both sides. These ureters may fuse into a
single duct anywhere along their course or open separately into the bladder
(where the upper ureter enters below the lower ureter).