
Page 413 - Clinical Application of Mechanical Ventilation
P. 413
Management of Mechanical Ventilation 379
2002). Permissive hypercapnia is done by using a low ventilator tidal volume
in the range of 4–7 mL/kg (normally 10 mL/kg) (Feihl et al., 1994). The re-
duced tidal volume lowers the peak inspiratory pressure and minimizes pressure-
or volume-related complications. Since the plateau pressure (i.e., end-inspiratory
The plateau pressure occlusion pressure) is the best estimate of the average peak alveolar pressure, it
should be kept below at or
35 cm H 2 O to avoid pressure- is often used as the target pressure when trying to avoid alveolar overdistention
induced lung injuries. (Slutsky, 1994). The ventilator tidal volume may be titrated to keep the plateau
pressure at or below 35 cm H O.
2
Low tidal volume may cause hypoventilation, CO retention, and acidosis.
2
Acidosis leads to development of central nervous dysfunction, intracranial hyperten-
sion, neuromuscular weakness, cardiovascular impairment, and increased pulmo-
nary vascular resistance. These potential complications may be alleviated by keeping
the pH within its normal range (7.35–7.45), either by renal compensation over time
or by neutralizing the acid with bicarbonate or tromethamine (Marini, 1993).
Tromethamine (THAM) is a nonbicarbonate buffer that helps to compensate for
metabolic acidosis. THAM directly decreases the hydrogen ion concentration and
Tromethamine (THAM) indirectly decreases the carbon dioxide level. The beneficial result is an increased
lowers the carbon dioxide bicarbonate level. Because of its lowering effect on the carbon dioxide level,
level and increases the bicar-
bonate levels. It is preferable tromethamine may be preferable to bicarbonate in patients who are being managed
to bicarbonate in patients with permissive hypercapnia (Kallet et al., 2000). Dosage of 0.3 M tromethamine
undergoing permissive
hypercapnia. needed to compensate for metabolic acidosis is calculated by: body weight in Kg 3
base deficit in mEq/L. Side effects of tromethamine include transient hypoglycemia,
respiratory depression, and hemorrhagic hepatic necrosis (Nahas et al., 1998).
By normalizing the pH, it appears that permissive hypercapnia may be a safe and
beneficial strategy in the management of patients with status asthmaticus (Cox et al.,
1991; Darioli et al., 1984), and adult respiratory distress syndrome (ARDS) (Feihl
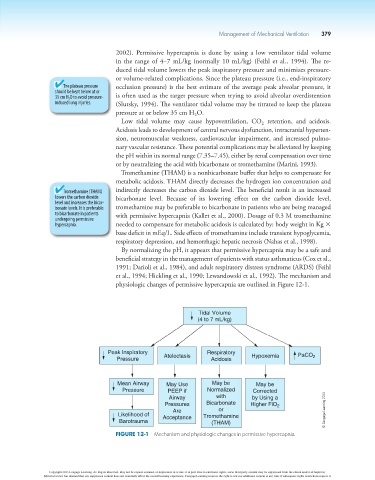
et al., 1994; Hickling et al., 1990; Lewandowski et al., 1992). The mechanism and
physiologic changes of permissive hypercapnia are outlined in Figure 12-1.
Tidal Volume
(4 to 7 mL/kg)
Peak Inspiratory Respiratory
Pressure Atelectasis Acidosis Hypoxemia PaCO 2
Mean Airway May Use May be May be
Pressure PEEP if Normalized Corrected
Airway with by Using a
Pressures Bicarbonate Higher FiO 2
Are or © Cengage Learning 2014
Likelihood of Acceptance Tromethamine
Barotrauma (THAM)
Figure 12-1 Mechanism and physiologic changes in permissive hypercapnia.
Copyright 2013 Cengage Learning. All Rights Reserved. May not be copied, scanned, or duplicated, in whole or in part. Due to electronic rights, some third party content may be suppressed from the eBook and/or eChapter(s).
Editorial review has deemed that any suppressed content does not materially affect the overall learning experience. Cengage Learning reserves the right to remove additional content at any time if subsequent rights restrictions require it.