
Page 242 - Cardiac Nursing
P. 242
0/0
6/2
0/0
3
3
6/2
1
0:4
1
009
009
xd
1-2
1-2
21
p
21
44.
q
xd
q
44.
q
A
p
A
18
18
p
ara
ara
t
p
t
e 2
M
M
6 A
0:4
6 A
Pa
g
e 2
g
Pa
g
K34
LWBK340-c10_
10_
0-c
LWB
LWB K34 0-c 10_ p pp211-244.qxd 30/06/2009 10:46 AM Page 218 Aptara
218 P A R T III / Assessment of Heart Disease
37 C (98.6 F). However, there is a diurnal pattern of temperature A Corneal Arcus
fluctuation, with temperatures as low as 35.8 C (96.4 F) orally in
the early morning to as high as 37.3 C (99.1 F) orally in the late af-
ternoon or evening. Oral temperatures average 0.5 C (1.0 F) lower
8
than rectal temperatures, but this difference is quite variable. Nor-
malbody temperature may be less than 37 C in older adults be-
cause of reducedheat production (lower metabolic activity, less
muscle mass and activity) and conservation (less insulation). 15
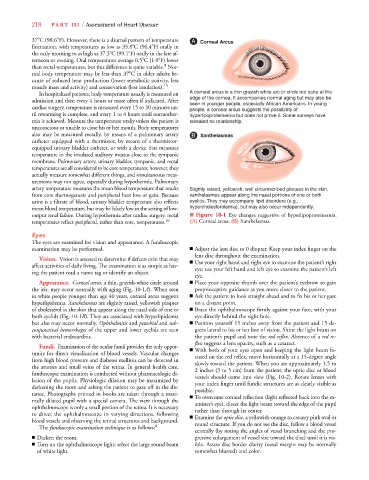
In hospitalized patients, body temperature usually is measured on A corneal arcus is a thin grayish white arc or circle not quite at the
admission and then every 4 hours or more often if indicated. After edge of the cornea. It accompanies normal aging but may also be
seen in younger people, especially African Americans. In young
cardiac surgery, temperature is measured every 15 to 30 minutes un-
people, a corneal arcus suggests the possibility of
til rewarming is complete, and every 1 to 4 hours until normother- hyperlipoproteinemia but does not prove it. Some surveys have
mia is achieved. Measure the temperature orally unless the patient is revealed no relationship.
unconscious or unable to close his or her mouth. Body temperatures
also may be measured rectally, by means of a pulmonary artery B Xanthelasmas
y
catheter equipped with a thermistor, by means of a thermistor-
equipped urinary bladder catheter, or with a device that measures
temperature in the insulated auditory meatus close to the tympanic
membrane. Pulmonary artery, urinary bladder, tympanic, and rectal
temperatures are all considered to be core temperatures; however, they
actually measure somewhat different things, and simultaneous meas-
urements may not agree, especially during hypothermia. Pulmonary
artery temperature measures the mean blood temperature that results Slightly raised, yellowish, well circumscribed plaques in the skin,
from core thermogenesis and peripheral heat loss or gain. Because xanthelasmas appear along the nasal portions of one or both
urine is a filtrate of blood, urinary bladder temperature also reflects eyelids. They may accompany lipid disorders (e.g.,
mean blood temperature, but may be falsely low in the setting of low- hypercholesterolemia), but may also occur independently.
output renal failure. During hypothermia after cardiac surgery, rectal ■ Figure 10-1 Eye changes suggestive of hyperlipoproteinemia.
temperatures reflect peripheral, rather than core, temperatures. 16 (A) Corneal arcus. (B) Xanthelasmas.
Eyes
The eyes are examinedfor vision and appearance. A funduscopic
examination may be performed. ■ Adjust the lens disc to 0 diopter. Keep your index finger on the
lens disc throughout the examination.
Vision. Vision is assessed to determine if defects exist that may
■ Use your right hand and right eye to examine the patient’s right
affect activities of daily living. The examination is as simple as hav- eye; use your left hand and left eye to examine the patient’s left
ing the patient read a name tag or identify an object.
eye.
Appearance. Corneal arcus, a thin, grayish-white circle around ■ Place your opposite thumb over the patient’s eyebrow to gain
the iris, may occur normally with aging (Fig. 10-1A). When seen proprioceptive guidance as you move closer to the patient.
in white people younger than age 40 years, corneal arcus suggests ■ Ask the patient to look straight ahead and to fix his or her gaze
hyperlipidemia. Xanthelasmas are slightly raised, yellowish plaques on a distant point.
of cholesterol in the skin that appear along the nasal side of one or ■ Brace the ophthalmoscope firmly against your face, with your
both eyelids (Fig. 10-1B). They are associated with hyperlipidemia eye directly behind the sight hole.
B
but also may occur normally. Ophthalmitis and petechial and sub- ■ Position yourself 15 inches away from the patient and 15 de-
conjunctivalhemorrhages of the upper andlower eyelids are seen grees lateral to his or her line of vision. Shine the light beam on
withbacterial endocarditis. the patient’s pupil and note the red reflex. Absence of a red re-
flex suggests a lens opacity, such as a cataract.
Fundi. Examination of the ocular fundi provides the only oppor- ■ With both of your eyes open and keeping the light beam fo-
tunity for direct visualization of blood vessels. Vascular changes
cused on the red reflex, move horizontally at a 15-degree angle
from high blood pressure and diabetes mellitus can be detected in slowly toward the patient. When you are approximately 1.5 to
the arteries and small veins of the retina. In general health care,
2 inches (3 to 5 cm) from the patient, the optic disc or blood
funduscopic examination is conducted without pharmacologic di- vessels should come into view (Fig. 10-2). Rotate lenses with
lation of the pupils. Physiologic dilation may be maximized by
your index finger until fundic structures are as clearly visible as
darkening the room and asking the patient to gaze off in the dis- possible.
tance. Photographs printed in books are taken through a maxi-
■ To overcome corneal reflection (light reflected back into the ex-
mally dilated pupil with a special camera. The view through the aminer’s eye), direct the light beam toward the edge of the pupil
ophthalmoscope is only a small portion of the retina. It is necessary
rather than through its center.
to direct the ophthalmoscope in varying directions, following ■ Examine the optic disc, a yellowish-orange to creamy pink oval or
blood vessels and observing the retinal structures and background. round structure. If you do not see the disc, follow a blood vessel
The funduscopic examination technique is as follows: 8
centrally (by noting the angles of vessel branching and the pro-
■ Darken the room. gressive enlargement of vessel size toward the disc) until it is vis-
■ Turn on the ophthalmoscope light; select the large round beam ible. Assess disc border clarity (nasal margin may be normally
of white light. somewhat blurred) and color.