
Page 265 - Cardiac Nursing
P. 265
6/2
009
6/2
0/0
0/0
0:4
0:4
1
009
1
3
44.
q
44.
1-2
1-2
xd
3
xd
q
q
7 A
p
p
A
41
A
ara
ara
t
p
t
41
Pa
Pa
M
7 A
M
e 2
e 2
g
g
g
LWBK340-c10_
LWB
p
10_
0-c
K34
21
LWB K34 0-c 10_ pp211-244.qxd 30/06/2009 10:47 AM Page 241 Aptara
p
21
C HAPTER 1 0 / History Taking and Physical Examination 241
Table 10-8 ■ PERCUSSION NOTES AND THEIR CHARACTERISTICS
Relative Intensity Relative Pitch Relative Duration Example of Location
Flatness Soft High Short Thigh
Dullness Medium Medium Medium Liver
Resonance Loud Low Long Normal lung
Hyperresonance Very loud Lower Longer None normally
Tympany Loud High * * Gastric air bubble or puffed-
out cheek
*Distinguished mainly by its musical timbre.
Bickley, L. S., & Szilagyi, P. G. (2009). Bates’ guide to physical examination and history taking (10th ed.). Philadelphia: Lippincott Williams & Wilkins.
replaces resonance when fluid or solid tissue replaces air-filled tis- Bronchial sounds, heard normally over the bronchial areas, are
sue. In patients with emphysema and air trapping, hyper-resonance loud and high pitched. Expiratory time is greater than inspira-
replaces resonance. Diaphragmatic excursion can be ascertained by tory time. If heard in the lung periphery, bronchial sounds are
percussion of the border between resonance (lung tissue) and dull- abnormal.
ness (muscle) in expiration and inspiration. Normal excursion is Adventitious breath sounds are superimposed over normal
5 to 6 cm. breath sounds. There are two categories of adventitious sounds:
discontinuous (crackles) and continuous (wheezes and pleural
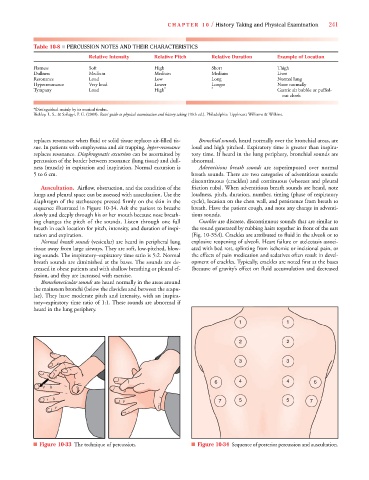
Auscultation. Airflow, obstruction, and the condition of the friction rubs). When adventitious breath sounds are heard, note
lungs and pleural space can be assessed with auscultation. Use the loudness, pitch, duration, number, timing (phase of respiratory
diaphragm of the stethoscope pressed firmly on the skin in the cycle), location on the chest wall, and persistence from breath to
sequence illustrated in Figure 10-34. Ask the patient to breathe breath. Have the patient cough, and note any change in adventi-
slowly and deeply through his or her mouth because nose breath- tious sounds.
ing changes the pitch of the sounds. Listen through one full Crackles are discrete, discontinuous sounds that are similar to
breath in each location for pitch, intensity, and duration of inspi- the sound generated by rubbing hairs together in front of the ears
ration and expiration. (Fig. 10-35A). Crackles are attributed to fluid in the alveoli or to
Normal breath sounds (vesicular) are heard in peripheral lung explosive reopening of alveoli. Heart failure or atelectasis associ-
tissue away from large airways. They are soft, low-pitched, blow- ated with bed rest, splinting from ischemic or incisional pain, or
ing sounds. The inspiratory–expiratory time ratio is 5:2. Normal the effects of pain medication and sedatives often result in devel-
breath sounds are diminished at the bases. The sounds are de- opment of crackles. Typically, crackles are noted first at the bases
creased in obese patients and with shallow breathing or pleural ef- (because of gravity’s effect on fluid accumulation and decreased
fusion, and they are increased with exercise.
Bronchovesicular sounds are heard normally in the areas around
the mainstem bronchi (below the clavicles and between the scapu-
lae). They have moderate pitch and intensity, with an inspira-
tory–expiratory time ratio of 1:1. These sounds are abnormal if
heard in the lung periphery.
1 1
2 2
3 3
6 4 4 6
7 5 5 7
■ Figure 10-33 The technique of percussion. ■ Figure 10-34 Sequence of posterior percussion and auscultation.