
Page 581 - Cardiac Nursing
P. 581
009
009
6/2
0/0
6/2
1:4
3 P
1:4
0
0
0/0
q
q
q
94.
94.
3
3
3
xd
xd
p
p
A
57
A
ara
ara
t
p
t
57
Pa
Pa
M
3 P
M
e 5
e 5
g
g
g
p
p
24_
24_
5-5
5-5
55
55
LWB
K34
LWBK340-c24_ pp555-594.qxd 30/06/2009 01:43 PM Page 557 Aptara
LWB
0-c
0-c
K34
C HAPTER 24 / Heart Failure and Cardiogenic Shock 557
At Risk for Heart Failure Heart Failure
Stage A Stage B Stage C
At high risk for HF Structural heart Structural heart Stage D
Refractory HF
but without structural disease but without disease with prior or requiring specialized
heart disease or signs or symptoms current symptoms interventions
symptoms of HF of HF of HF
e.g.: Patients
e.g.: Patients with:
e.g.: Patients with: who have marked
-hypertension e.g.: Patients with: -known structural symptoms at rest
-atherosclerotic -previous MI
S Sttruucctuurral D D Deeveloppmmennt t heart disease R Refaactory y despite maximal
v
e
c
o
r
o
a
t
m
e
e
disease -LV remodeling
o
h heeearrt o of ssyymptomms s and s syymppttommss ooff medical therapy
m
m
m
a
m
p
m
o
-diabetes including LVH and
s
s
s
d diseeaase e e o off HF F -shortness of H HFF aatt reest (e.g., those who are
e
H
-obesity low EF
breath and fatigue, recurrently
-metabolic syndrome -asymptomatic reduced exercise hospitalized or
or valvular disease tolerance cannot be safely
Patients discharged from
-using cardiotoxins the hospital without
-with FHx specialized
cardiomyopathy interventions)
Therapy Therapy Therapy Therapy
Goals Goals Goals Goals
-Treat hypertension -All measures under -All measures under stages -Appropriate measures
-Encourage smoking stage A A and B under stages A, B, C
cessation -Dietary salt restriction -Decision re: appropriate
g
-Treat lipid disorders Drugs Drugs for routine use level of care
g
-Encourage regular -ACEI or ARB in -Diuretics for fluid retention
p
exercise appropriate patients -ACEI Options
-Discourage alcohol (see text) -Beta-blockers -Compassionate end-of-
intake, illicit drug use -Beta-blockers in life care/hospice
g
p
-Control metabolic appropriate patients Drugs in selected patients -Extraordinary measures
syndrome (see text) -Aldosterone antagonist • heart transplant
Drugs -ARBs • chronic inotropes
g
-Digitalis • permanent mechanical
-ACEI or ARB in -Hydralazine/nitrates support
appropriate patients • experimental surgery
p
(see text) for vascular Devices in selected patients or drugs
disease or diabetes -Biventricular pacing
-Implantable defibrillators
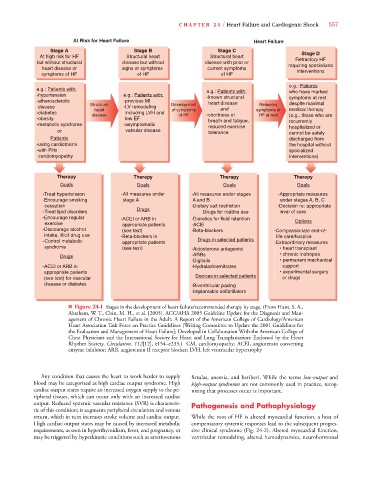
■ Figure 24-1 Stages in the development of heart failure/recommended therapy by stage. (From Hunt, S. A.,
Abraham, W. T., Chin, M. H., et al. [2005]. ACC/AHA 2005 Guideline Update for the Diagnosis and Man-
agement of Chronic Heart Failure in the Adult: A Report of the American College of Cardiology/American
Heart Association Task Force on Practice Guidelines [Writing Committee to Update the 2001 Guidelines for
the Evaluation and Management of Heart Failure]: Developed in Collaboration With the American College of
Chest Physicians and the International Society for Heart and Lung Transplantation: Endorsed by the Heart
Rhythm Society. Circulation, 112[12], e154–e235.) CM, cardiomyopathy; ACEI, angiotensin converting
enzyme inhibitor; ARB, angiotensin II receptor blocker; LVH, left ventricular hypertrophy
Any condition that causes the heart to work harder to supply fistulas, anemia, and beriberi. While the terms low-output and
blood may be categorized as high cardiac output syndrome. High high-output syndromes are not commonly used in practice, recog-
cardiac output states require an increased oxygen supply to the pe- nizing that processes occur is important.
ripheral tissues, which can occur only with an increased cardiac
output. Reduced systemic vascular resistance (SVR) is characteris- Pathogenesis and Pathophysiology
tic of this condition; it augments peripheral circulation and venous
return, which in turn increases stroke volume and cardiac output. While the root of HF is altered myocardial function, a host of
High cardiac output states may be caused by increased metabolic compensatory systemic responses lead to the subsequent progres-
requirements, as seen in hyperthyroidism, fever, and pregnancy, or sive clinical syndrome (Fig. 24-2). Altered myocardial function,
may be triggered by hyperkinetic conditions such as arteriovenous ventricular remodeling, altered hemodynamics, neurohormonal