
Page 633 - Cardiac Nursing
P. 633
1
1
009
009
7:4
5
Pa
7:4
5
0/2
xd
0
q
xd
0
6/3
0/2
0
6/3
p
p
A
A
p
ara
ara
t
t
A
g
g
Pa
Pa
g
09
09
e 6
e 6
q
K34
LWBK340-c25_
LWB
0-c
59
59
25_
22.
22.
q
LWB K34 0-c 25_ p p pp595-622.qxd 06/30/2009 17:45 Page 609 Aptara
5-6
5-6
C HAPTER 2 5 / Cardiac Surgery 609
(performed when recipients are accepted as transplantation candi- An alternative technique is referred to as total orthotopic heart
dates) against standard pools of lymphocytes from multiple serum transplantation or the bicaval and pulmonary venous anastomo-
donors. This result is reported in a percentage of panel reactive an- sis. The basic features of the bicaval method are complete excision
tibody (% PRA). Patients with a known positive reaction, a positive of the recipient atria and donor heart implantation with bicaval
PRA for example of 50%, will have additional HLA testing to iden- end-to-end anastomosis. Proponents of this technique cite the po-
tify those specific circulating antibodies. These candidates are iden- tential for more synchronous atrial contraction, and reduction of
tified as “sensitized” such that the candidates antibodies could react pacemaker implantation and atrioventricular valve regurgita-
to certain donor cell antigens and result in antibody-mediated tion. 65
rejection. Therapies are available to reduce these antibodies.
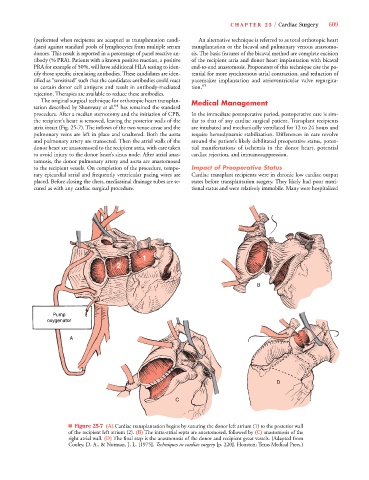
The original surgical technique for orthotopic heart transplan- Medical Management
tation described by Shumway et al. 64 has remained the standard
procedure. After a median sternotomy and the initiation of CPB, In the immediate postoperative period, postoperative care is sim-
the recipient’s heart is removed, leaving the posterior walls of the ilar to that of any cardiac surgical patient. Transplant recipients
atria intact (Fig. 25-7). The inflows of the two venae cavae and the are intubated and mechanically ventilated for 12 to 24 hours and
pulmonary veins are left in place and unaltered. Both the aorta require hemodynamic stabilization. Differences in care revolve
and pulmonary artery are transected. Then the atrial walls of the around the patient’s likely debilitated preoperative status, poten-
donor heart are anastomosed to the recipient atria, with care taken tial manifestations of ischemia in the donor heart, potential
to avoid injury to the donor heart’s sinus node. After atrial anas- cardiac rejection, and immunosuppression.
tomosis, the donor pulmonary artery and aorta are anastomosed
to the recipient vessels. On completion of the procedure, tempo- Impact of Preoperative Status
rary epicardial atrial and frequently ventricular pacing wires are Cardiac transplant recipients were in chronic low cardiac output
placed. Before closing the chest, mediastinal drainage tubes are se- states before transplantation surgery. They likely had poor nutri-
cured as with any cardiac surgical procedure. tional status and were relatively immobile. Many were hospitalized
1
2
B
Pump
oxygenator
A
D
C
■ Figure 25-7 (A) Cardiac transplantation begins by suturing the donor left atrium (1) to the posterior wall
of the recipient left atrium (2). (B) The intra-atrial septa are anastomosed, followed by (C) anastomosis of the
right atrial wall. (D) The final step is the anastomosis of the donor and recipient great vessels. (Adapted from
Cooley, D. A., & Norman, J. L. [1975]. Techniques in cardiac surgery [p. 220]. Houston: Texas Medical Press.)