
Page 673 - Cardiac Nursing
P. 673
M
M
1 A
2:0
1 A
g
g
Pa
Pa
Pa
2:0
/30
/09
/30
6
6
1
1
1
/09
/09
ara
a
ara
t
t
c.
c.
In
a
In
p
49
49
e 6
g
e 6
p
p
A
49
A
p
63
LWBK340-c27_ pp638-654.qxd 6/30/09 12:01 AM Page 649 Aptara Inc.
p
8-6
54.
63
8-6
LWB
27_
0-c
27_
27_
K34
LWB
0-c
K34
54.
q
xd
q
q
xd
54.
C HAPTER 2 7 / Sudden Cardiac Death and Cardiac Arrest 649
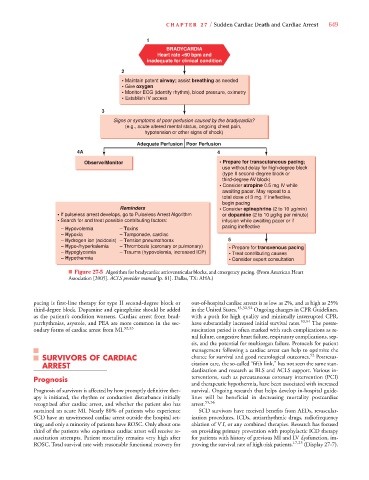
1
BRADYCARDIA
Heart rate <60 bpm and
inadequate for clinical condition
2
• Maintain patent airway; assist breathing as needed
• Give oxygen
• Monitor ECG (identify rhythm), blood pressure, oximetry
• Establish IV access
3
Signs or symptoms of poor perfusion caused by the bradycardia?
(e.g., acute altered mental status, ongoing chest pain,
hypotension or other signs of shock)
Adequate Perfusion Poor Perfusion
4A 4
Observe/Monitor • Prepare for transcutaneous pacing;
use without delay for high-degree block
(type II second-degree block or
third-degree AV block)
• Consider atropine 0.5 mg IV while
awaiting pacer. May repeat to a
total dose of 3 mg. If ineffective,
begin pacing
Reminders • Consider epinephrine (2 to 10 μg/min)
• If pulseless arrest develops, go to Pulseless Arrest Algorithm or dopamine (2 to 10 μg/kg per minute)
• Search for and treat possible contributing factors: infusion while awaiting pacer or if
pacing ineffective
– Hypovolemia – Toxins
– Hypoxia – Tamponade, cardiac
– Hydrogen ion (acidosis) – Tension pneumothorax 5
– Hypo-/hyperkalemia – Thrombosis (coronary or pulmonary) • Prepare for transvenous pacing
– Hypoglycemia – Trauma (hypovolemia, increased ICP) • Treat contributing causes
– Hypothermia • Consider expert consultation
■ Figure 27-5 Algorithm for bradycardia: atrioventricular blocks, and emergency pacing. (From American Heart
Association [2005]. ACLS provider manual [p. 81]. Dallas, TX: AHA.)
pacing is first-line therapy for type II second-degree block or out-of-hospital cardiac arrests is as low as 2%, and as high as 25%
third-degree block. Dopamine and epinephrine should be added in the United States. 13,32,52 Ongoing changes in CPR Guidelines,
as the patient’s condition worsens. Cardiac arrest from brad- with a push for high quality and minimally interrupted CPR,
yarrhythmias, asystole, and PEA are more common in the sec- have substantially increased initial survival rates. 53,54 The postre-
ondary forms of cardiac arrest from MI. 32,33 suscitation period is often marked with such complications as re-
nal failure, congestive heart failure, respiratory complications, sep-
sis, and the potential for multiorgan failure. Protocols for patient
management following a cardiac arrest can help to optimize the
SURVIVORS OF CARDIAC chance for survival and good neurological outcomes. 52 Postresus-
ARREST citation care, the so-called “fifth link,” has not seen the same stan-
dardization and research as BLS and ACLS support. Various in-
Prognosis terventions, such as percutaneous coronary intervention (PCI)
and therapeutic hypothermia, have been associated with increased
Prognosis of survivors is affected by how promptly definitive ther- survival. Ongoing research that helps develop in-hospital guide-
apy is initiated, the rhythm or conduction disturbance initially lines will be beneficial in decreasing mortality postcardiac
recognized after cardiac arrest, and whether the patient also has arrest. 55,56
sustained an acute MI. Nearly 80% of patients who experience SCD survivors have received benefits from AEDs, revascular-
SCD have an unwitnessed cardiac arrest outside the hospital set- ization procedures, ICDs, antiarrhythmic drugs, radiofrequency
ting; and only a minority of patients have ROSC. Only about one ablation of VT, or any combined therapies. Research has focused
third of the patients who experience cardiac arrest will receive re- on providing primary prevention with prophylactic ICD therapy
suscitation attempts. Patient mortality remains very high after for patients with history of previous MI and LV dysfunction, im-
ROSC. Total survival rate with reasonable functional recovery for proving the survival rate of high-risk patients. 17,23 (Display 27-7).