
Page 257 - ACCCN's Critical Care Nursing
P. 257
234 P R I N C I P L E S A N D P R A C T I C E O F C R I T I C A L C A R E
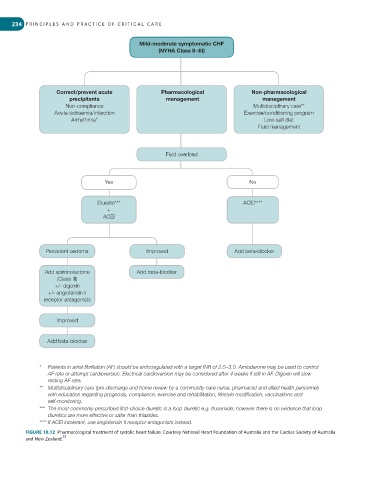
Mild-moderate symptomatic CHF
(NYHA Class II – III)
Correct/prevent acute Pharmacological Non-pharmacological
precipitants management management
Non-compliance Multidisciplinary care**
Acute ischaemia/infarction Exercise/conditioning program
Arrhythmia* Low-salt diet
Fluid management
Fluid overload
Yes No
Diuretic*** ACEI****
+
ACEI
Persistent oedema Improved Add beta-blocker
Add spironolactone Add beta-blocker
(Class III)
+/- digoxin
+/- angiotensin II
receptor antagonists
Improved
Add beta-blocker
* Patients in atrial fi brillation (AF) should be anticoagulated with a target INR of 2.0 – 3.0. Amiodarone may be used to control
AF rate or attempt cardioversion. Electrical cardioversion may be considered after 4 weeks if still in AF. Digoxin will slow
resting AF rate.
** Multidisciplinary care (pre-discharge and home review by a community care nurse, pharmacist and allied health personnel)
with education regarding prognosis, compliance, exercise and rehabilitation, lifestyle modifi cation, vaccinations and
self-monitoring.
*** The most commonly prescribed fi rst-choice diuretic is a loop diuretic e.g. frusemide; however there is no evidence that loop
diuretics are more effective or safer than thiazides.
**** If ACEI intolerant, use angiotensin II receptor antagonists instead.
FIGURE 10.12 Pharmacological treatment of systolic heart failure. Courtesy National Heart Foundation of Australia and the Cardiac Society of Australia
55
and New Zealand.