
Page 116 - Concise Pathology for Exam Preparation ( PDFDrive )
P. 116
5 Diseases of Immunity 101
(b)
Small- and medium-sized complexes have antigen excess, are cleared less effec-
tively and are the most pathogenic complexes.
2.
Functional status of mononuclear phagocytic system (MPS): Intrinsic dysfunction or
overload of MPS increases the probability of persistence of immune complexes in cir-
culation and tissue deposition.
Charge of immune complex
3.
The three-dimensional structure of immune complex
4.
5.
Valency of the antigen
Affinity of the antigen to tissue components and avidity of antibody
6.
Haemodynamic factors
7.
Favoured Sites of Deposition
Renal glomeruli, joints, skin, heart, serosa and small blood vessels.
Morphology of Immune Complex-Mediated Tissue Injury
• Necrotizing vasculitis (fibrinoid necrosis and neutrophils in the vessel wall)
• Swelling and proliferation of endothelial and mesangial cells
• Neutrophilic and monocytic infiltration into glomeruli
• Hypercellular glomeruli
• Immunofluorescence: granular lumpy deposits of immunoglobulins and complement
• Electron microscopy: electron-dense deposits
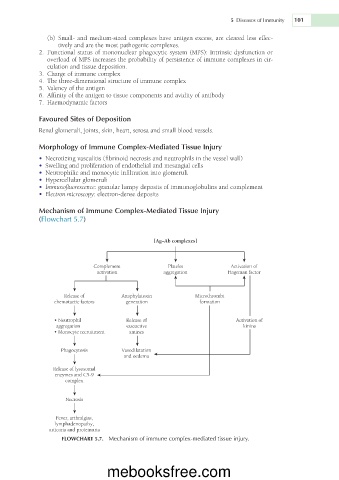
Mechanism of Immune Complex-Mediated Tissue Injury
(Flowchart 5.7)
[Ag–Ab complexes]
Complement Platelet Activation of
activation aggregation Hageman factor
Release of Anaphylatoxin Microthrombi
chemotactic factors generation formation
• Neutrophil Release of Activation of
aggregation vasoactive kinins
• Monocyte recruitment amines
Phagocytosis Vasodilatation
and oedema
Release of lysosomal
enzymes and C59
complex
Necrosis
Fever, arthralgias,
lymphadenopathy,
urticaria and proteinuria
FLOWCHART 5.7. Mechanism of immune complex-mediated tissue injury.
mebooksfree.com