
Page 380 - Concise Pathology for Exam Preparation ( PDFDrive )
P. 380
13 The Lung 365
presentation of bronchiectasis, while the latter is most often associated with systemic
illnesses.
• The bronchi and bronchioles are dilated and can be traced up to the pleural surface.
• The wall of the bronchi is thickened due to fibrosis and the lumen may be filled with
mucopurulent secretions.
• Reid characterized bronchiectasis as cylindrical, cystic or varicose based on mor-
phology:
• Cylindrical bronchiectasis: Bronchi are dilated minimally and have straight, regular
outlines (primarily due to mucosal oedema)
• Cystic or saccular bronchiectasis: Bronchi have a ballooned appearance and demon-
strate air-fluid levels (due to ulceration with bronchial neovascularization).
• Varicose bronchiectasis: Bulbous bronchi with dilatations and intervening sites of
relative constriction due to scarring.
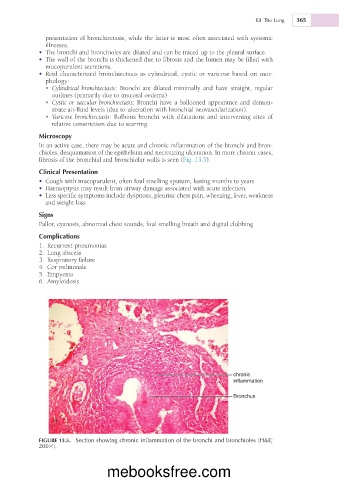
Microscopy
In an active case, there may be acute and chronic inflammation of the bronchi and bron-
chioles, desquamation of the epithelium and necrotizing ulceration. In more chronic cases,
fibrosis of the bronchial and bronchiolar walls is seen (Fig. 13.5).
Clinical Presentation
• Cough with mucopurulent, often foul smelling sputum, lasting months to years
• Haemoptysis may result from airway damage associated with acute infection.
• Less specific symptoms include dyspnoea, pleuritic chest pain, wheezing, fever, weakness
and weight loss
Signs
Pallor, cyanosis, abnormal chest sounds, foul smelling breath and digital clubbing
Complications
1. Recurrent pneumonias
2. Lung abscess
3. Respiratory failure
4. Cor pulmonale
5. Empyema
6. Amyloidosis
chronic
inflammation
Bronchus
FIGURE 13.5. Section showing chronic inflammation of the bronchi and bronchioles (H&E;
2003).
mebooksfree.com