
Page 554 - Concise Pathology for Exam Preparation ( PDFDrive )
P. 554
20 Endocrinology 539
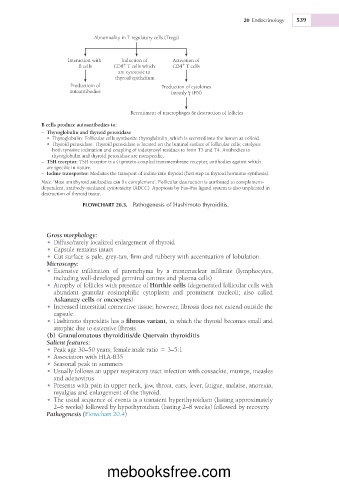
Abnormality in T regulatory cells (Tregs)
Interaction with Induction of Activation of
+
+
B cells CD8 T cells which CD4 T cells
are cytotoxic to
thyroid epithelium
Productioin of Production of cytokines
autoantibodies (mainly γ IFN)
Recruitment of macrophages & destruction of follicles
B cells produce autoantibodies to:
– Thyroglobulin and thyroid peroxidase
• Thyroglobulin: Follicular cells synthesize thyroglobulin, which is secreted into the lumen as colloid.
• Thyroid peroxidase: Thyroid peroxidase is located on the luminal surface of follicular cells; catalyses
both tyrosine iodination and coupling of iodotyrosyl residues to form T3 and T4. Antibodies to
thyroglobulin and thyroid peroxidase are nonspecific.
– TSH receptor: TSH receptor is a G protein-coupled transmembrane receptor, antibodies against which
are specific in nature.
– Iodine transporter: Mediates the transport of iodine into thyroid (first step in thyroid hormone synthesis).
Note: ‘Most antithyroid antibodies can fix complement’. Follicular destruction is attributed to complement-
dependent, antibody-mediated cytotoxicity (ADCC). Apoptosis by Fas–Fas ligand system is also implicated in
destruction of thyroid tissue.
FLOWCHART 20.3. Pathogenesis of Hashimoto thyroiditis.
Gross morphology:
• Diffuse/rarely localized enlargement of thyroid
• Capsule remains intact
• Cut surface is pale, grey-tan, firm and rubbery with accentuation of lobulation.
Microscopy:
• Extensive infiltration of parenchyma by a mononuclear infiltrate (lymphocytes,
including well-developed germinal centres and plasma cells)
• Atrophy of follicles with presence of Hürthle cells (degenerated follicular cells with
abundant granular eosinophilic cytoplasm and prominent nucleoli; also called
Askanazy cells or oncocytes)
• Increased interstitial connective tissue; however, fibrosis does not extend outside the
capsule.
• Hashimoto thyroiditis has a fibrous variant, in which the thyroid becomes small and
atrophic due to extensive fibrosis.
(b) Granulomatous thyroiditis/de Quervain thyroiditis
Salient features:
• Peak age 30–50 years; female:male ratio 5 3–5:1
• Association with HLA-B35
• Seasonal peak in summers
• Usually follows an upper respiratory tract infection with coxsackie, mumps, measles
and adenovirus
• Presents with pain in upper neck, jaw, throat, ears, fever, fatigue, malaise, anorexia,
myalgias and enlargement of the thyroid.
• The usual sequence of events is a transient hyperthyroidism (lasting approximately
2–6 weeks) followed by hypothyroidism (lasting 2–8 weeks) followed by recovery.
Pathogenesis (Flowchart 20.4)
mebooksfree.com