
Page 1451 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 1451
Chapter 80 Clinical Manifestations, Staging, and Treatment of Follicular Lymphoma 1291
1.00 1.00
Cumulative survival 0.75 Cumulative risk of transformation 0.75 N = 547
0.50
0.50
0.25
transformation
in 151
N = 547 0.25 Documented
0.00 0.00
0 10 20 30 40 0 10 20 30
Years from diagnosis Years from diagnosis
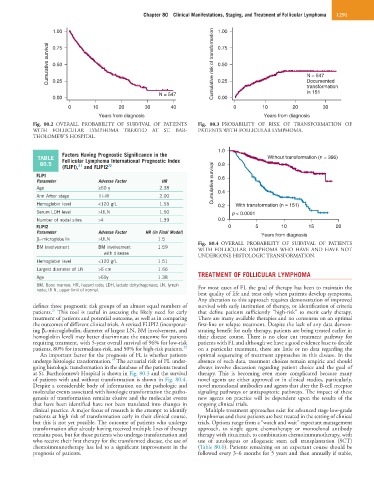
Fig. 80.2 OVERALL PROBABILITY OF SURVIVAL OF PATIENTS Fig. 80.3 PROBABILITY OF RISK OF TRANSFORMATION OF
WITH FOLLICULAR LYMPHOMA TREATED AT ST. BAR- PATIENTS WITH FOLLICULAR LYMPHOMA.
THOLOMEW’S HOSPITAL.
1.0
Factors Having Prognostic Significance in the
TABLE Follicular Lymphoma International Prognostic Index Without transformation (n = 396)
80.5 0.8
(FLIPI), and FLIPI2 22
21
FLIPI 0.6
Parameter Adverse Factor HR Cumulative survival
Age ≥60 y 2.38 0.4
Ann Arbor stage III–IV 2.00
Hemoglobin level <120 g/L 1.55 0.2 With transformation (n = 151)
Serum LDH level >ULN 1.50 p < 0.0001
Number of nodal sites >4 1.39 0.0
FLIPI2 0 5 10 15 20
Parameter Adverse Factor HR (in Final Model) Years from diagnosis
β 2 -microglobulin >ULN 1.5
BM involvement BM involvement 1.59 Fig. 80.4 OVERALL PROBABILITY OF SURVIVAL OF PATIENTS
WITH FOLLICULAR LYMPHOMA WHO HAVE AND HAVE NOT
with disease UNDERGONE HISTOLOGIC TRANSFORMATION.
Hemoglobin level <120 g/L 1.51
Largest diameter of LN >6 cm 1.66
Age >60y 1.38 TREATMENT OF FOLLICULAR LYMPHOMA
BM, Bone marrow; HR, hazard ratio; LDH, lactate dehydrogenase; LN, lymph For most cases of FL the goal of therapy has been to maintain the
node; ULN, upper limit of normal.
best quality of life and treat only when patients develop symptoms.
Any alteration to this approach requires demonstration of improved
defines three prognostic risk groups of an almost equal numbers of survival with early institution of therapy, or identification of criteria
21
patients. This tool is useful in assessing the likely need for early that define patients sufficiently “high-risk” to merit early therapy.
treatment of patients and potential outcome, as well as in comparing There are many available therapies and no consensus on an optimal
the outcomes of different clinical trials. A revised FLIPI2 (incorporat- first-line or relapse treatment. Despite the lack of any data demon-
ing β 2 -microglobulin, diameter of largest LN, BM involvement, and strating benefit for early therapy, patients are being treated earlier in
hemoglobin level) may better discriminate the outcome for patients their disease course. There is no clear cut treatment pathway for
requiring treatment, with 5-year overall survival of 96% for low-risk patients with FL and although we have a good evidence base to decide
patients, 80% for intermediate-risk, and 50% for high-risk patients. 22 on a particular treatment, there are little or no data regarding the
An important factor for the prognosis of FL is whether patients optimal sequencing of treatment approaches in this disease. In the
14
undergo histologic transformation. The actuarial risk of FL under- absence of such data, treatment choices remain empiric and should
going histologic transformation in the database of the patients treated always involve discussion regarding patient choice and the goal of
at St. Bartholomew’s Hospital is shown in Fig. 80.3 and the survival therapy. This is becoming even more complicated because many
of patients with and without transformation is shown in Fig. 80.4. novel agents are either approved or in clinical studies, particularly,
Despite a considerable body of information on the pathologic and novel monoclonal antibodies and agents that alter the B-cell receptor
molecular events associated with histologic transformation the patho- signaling pathways or antiapoptotic pathways. The impact of these
genesis of transformation remains elusive and the molecular events new agents on practice will be dependent upon the results of the
that have been identified have not been translated into changes in ongoing clinical trials.
clinical practice. A major focus of research is the attempt to identify Multiple treatment approaches exist for advanced stage low-grade
patients at high risk of transformation early in their clinical course, lymphomas and these patients are best treated in the setting of clinical
but this is not yet possible. The outcome of patients who undergo trials. Options range from a “watch and wait” expectant management
transformation after already having received multiple lines of therapy approach, to single agent chemotherapy or monoclonal antibody
remains poor, but for those patients who undergo transformation and therapy with rituximab, to combination chemoimmunotherapy, with
who receive their first therapy for the transformed disease, the use of use of autologous or allogeneic stem cell transplantation (SCT)
chemoimmunotherapy has led to a significant improvement in the (Table 80.6). Patients remaining on an expectant course should be
prognosis of patients. followed every 3–6 months for 5 years and then annually if stable,