
Page 607 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 607
516 Part V Red Blood Cells
Cbl-food protein
salivary R protein
Potential loci
for pathophysiology
Absorption of R-protein
Cbl CbI-food protein A. Nutritional: insufficient
Blood CbI intake.
CbI dissociated
from food by
Enterohepatic HCI acid proteolysis
circulation of CbI pepsin IF B. Abnormal intragastric
Biliary CbI and HCI Gastric events: poor dissociation
CbI analogues R-CbI Pepsin secretion of food-CbI.
excreted IF
CbI preferentially
R protein binds binds R protein C. Deficient or defective IF.
biliary CbI and R-CbI
CbI analogues
R-CbI Excess unbound
R-CbI analogues IF present
IF Food and biliary D. Abnormal events in
IF small bowel: Inadequate
R-CbI Pancreatic protease secreted CbI absorbed pancreatic protease.
Usurping of luminal CbI
IF CbI complex by bacteria or D. latum
IF-CbI resistant to TCII-CbI complex
Pancreatic protease IF-CbI CbI analogues proteolysis To portal blood and
selectively degrades systemic circulation
R proteins Degraded R protein IF receptors
E. Disordered mucosa and/or
Released CbI binds IF receptors and/or
IF within 10 minutes Ileum TCII-CbI transenterocytic transport.
IF receptors IF-CbI TCII-CbI
CbI analogues unbound IF-CbI IF-CbI TCII-CbI TCII binds CbI within enterocyte
IF-CbI IF
IF-CbI binds Ca 2+ receptor TCII CbI
IF receptors pH>5.4 TCII IF-CbI IF TCII
CbI analogues and CbI
degraded R proteins Enterocyte
are excreted
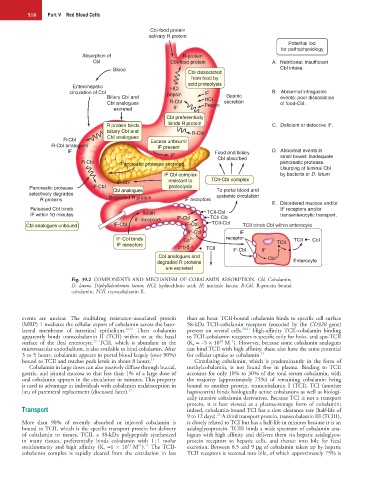
Fig. 39.2 COMPONENTS AND MECHANISM OF COBALAMIN ABSORPTION. Cbl, Cobalamin;
D. latum, Diphyllobothrium latum; HCl, hydrochloric acid; IF, intrinsic factor; R-Cbl, R-protein bound
cobalamin; TCII, transcobalamin II.
events are unclear. The multidrug resistance–associated protein than an hour. TCII-bound cobalamin binds to specific cell surface
(MRP) 1 mediates the cellular export of cobalamin across the baso- 58-kDa TCII-cobalamin receptors (encoded by the CD320 gene)
lateral membrane of intestinal epithelium. 18,19 Then cobalamin present on several cells. 20,21 High-affinity TCII-cobalamin binding
apparently binds transcobalamin II (TCII) within or at the basal to TCII-cobalamin receptors is specific only for holo- and apo-TCII
10
15
−1
surface of the ileal enterocyte. TCII, which is abundant in the (K a = ~5 × 10 M ). However, because some cobalamin analogues
microvascular endothelium, is also available to bind cobalamin. After can bind TCII with high affinity, these also have the same potential
3 to 5 hours, cobalamin appears in portal blood largely (over 90%) for cellular uptake as cobalamin. 15
bound to TCII and reaches peak levels in about 8 hours. 15 Circulating cobalamin, which is predominantly in the form of
Cobalamin in large doses can also passively diffuse through buccal, methylcobalamin, is not found free in plasma. Binding to TCII
gastric, and jejunal mucosa so that less than 1% of a large dose of accounts for only 10% to 30% of the total serum cobalamin, with
oral cobalamin appears in the circulation in minutes. This property the majority (approximately 75%) of remaining cobalamin being
is used to advantage in individuals with cobalamin malabsorption in bound to another protein, transcobalamin I (TCI). TCI (another
lieu of parenteral replacement (discussed later). 15 haptocorrin) binds biologically active cobalamins as well as biologi-
cally inactive cobalamin derivatives. Because TCI is not a transport
protein, it is best viewed as a plasma-storage form of cobalamin;
Transport indeed, cobalamin-bound TCI has a slow clearance rate (half-life of
22
9 to 12 days). A third transport protein, transcobalamin III (TCIII),
More than 90% of recently absorbed or injected cobalamin is is closely related to TCI but has a half-life in minutes because it is an
bound to TCII, which is the specific transport protein for delivery asialoglycoprotein. TCIII binds a wide spectrum of cobalamin ana-
of cobalamin to tissues. TCII, a 38-kDa polypeptide synthesized logues with high affinity and delivers them via hepatic asialoglyco-
in many tissues, preferentially binds cobalamin with 1 : 1 molar protein receptors to hepatic cells, and thence into bile for fecal
11
−1 15
stoichiometry and high affinity (K a =1 × 10 M ). The TCII- excretion. Between 0.5 and 9 µg of cobalamin taken up by hepatic
cobalamin complex is rapidly cleared from the circulation in less TCII receptors is secreted into bile, of which approximately 75% is