
Page 659 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 659
Chapter 40 Thalassemia Syndromes 561
requirement of more than 180–200 mL/kg/y of packed RBCs usually TABLE Survival by Birth Cohort at Different Ages of Patients
represents excessive RBC requirements. 330,331 For such patients, a 40.2 With Transfusion-Dependent Thalassemia
25% to 60% reduction in transfusion requirements after splenectomy
is generally predictable. Before attributing increased transfusion Patient Age Cohort (%)
requirements to hypersplenism, it is important to look for other (Years) 1970–1974 1975–1979 1980–1984
causes, such as RBC alloimmunization or a change in the hematocrit
52
of the units of donor blood. RBC survival studies using Cr-labeling 10 98 (96–99) 98 (96–99) 99 (95–100)
are not usually of value for predicting response to splenectomy. 15 95 (92–97) 97 (94–98) 98 (93–100)
Because of the greater risk of postsplenectomy sepsis in younger 20 89 (85–92) 96 (93–98)
patients, surgery should be deferred until after 5 years of age whenever
possible, so the humoral immune system has developed. For well- 25 82 (77–86)
transfused and well-chelated patients, splenectomy may have little Data from Borgna Pignatti C, Rugolotto S, De Stefano X, et al: Survival and
benefit, and some centers have noted a significant decline in the disease complications in thalassemia major. Ann N Y Acad Sci 850:227, 1998.
number of patients undergoing splenectomy in recent years.
Laparoscopic splenectomy has proved safe for patients with thalas-
semia and has dramatically shortened the recovery time compared
332
with open procedures. Partial splenectomy and partial dearterializa- 1.00
tion of the spleen have been suggested as alternative approaches to
reducing blood requirements without incurring the risk of sepsis. 333–335
The long-term benefits of this approach remain uncertain. Therapeu- 0.75
tic embolization of the spleen avoids the need for surgery, 336–338 but
this approach is frequently associated with postprocedure pain and
fever and does not permit the removal of accessory spleens. Proportion without cardiac disease 0.50
After splenectomy, striking thrombocytosis may occur, which may
339
require thrombosis prophylaxis or platelet deaggregating agents.
Increased numbers of nucleated RBCs appear in the blood, and the 0.25
presence of many RBCs containing inclusion bodies composed of
precipitated α-globin chains can be demonstrated by staining with
supravital staining.
Patients with thalassemia major are at significant risk for the 0.00
development of overwhelming, often fatal, infection after splenec- 0 2 4 6 8 10 12 14 16
340
tomy (postsplenectomy sepsis syndrome). The problem is most Years of chelation therapy
common in young children. Streptococcus pneumoniae causes two-
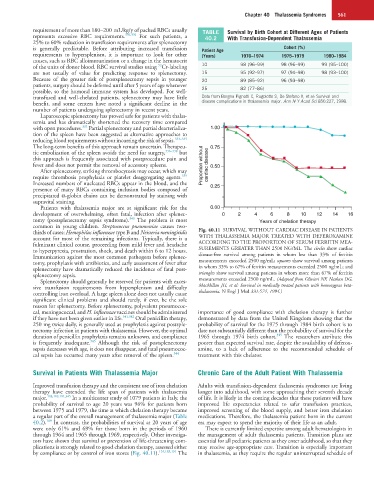
thirds of cases; Hemophilus influenzae type B and Neisseria meningitidis Fig. 40.11 SURVIVAL WITHOUT CARDIAC DISEASE IN PATIENTS
account for most of the remaining infections. Typically, there is a WITH THALASSEMIA MAJOR TREATED WITH DEFEROXAMINE
fulminant clinical course, proceeding from mild fever and headache ACCORDING TO THE PROPORTION OF SERUM FERRITIN MEA-
to hyperpyrexia, prostration, shock, and death within 6 to 12 hours. SUREMENTS GREATER THAN 2500 NG/ML. The circles show cardiac
Immunization against the most common pathogens before splenec- disease-free survival among patients in whom less than 33% of ferritin
tomy, prophylaxis with antibiotics, and early assessment of fever after measurements exceeded 2500 ng/mL; squares show survival among patients
splenectomy have dramatically reduced the incidence of fatal post- in whom 33% to 67% of ferritin measurements exceeded 2500 ng/mL; and
splenectomy sepsis. triangles show survival among patients in whom more than 67% of ferritin
Splenectomy should generally be reserved for patients with exces- measurements exceeded 2500 ng/mL. (Adapted from Olivieri NF, Nathan DG,
sive transfusion requirements from hypersplenism and difficulty MacMillan JH, et al: Survival in medically treated patients with homozygous beta-
controlling iron overload. A large spleen alone does not usually cause thalassemia. N Engl J Med 331:574, 1994.)
significant clinical problems and should rarely, if ever, be the sole
reason for splenectomy. Before splenectomy, polyvalent pneumococ-
cal, meningococcal, and H. influenzae vaccines should be administered importance of good compliance with chelation therapy is further
if they have not been given earlier in life. 341,342 Oral penicillin therapy, demonstrated by data from the United Kingdom showing that the
250 mg twice daily, is generally used as prophylaxis against postsple- probability of survival for the 1975 through 1984 birth cohort is to
nectomy infection in patients with thalassemia. However, the optimal date not substantially different than the probability of survival for the
345
duration of penicillin prophylaxis remains unknown, and compliance 1965 through 1974 birth cohort. The researchers attribute this
343
is frequently inadequate. Although the risk of postsplenectomy poorer than expected survival rate, despite the availability of deferox-
sepsis decreases with age, it does not disappear, and fatal pneumococ- amine, to a lack of adherence to the recommended schedule of
cal sepsis has occurred many years after removal of the spleen. 344 treatment with this chelator.
Survival in Patients With Thalassemia Major Chronic Care of the Adult Patient With Thalassemia
Improved transfusion therapy and the consistent use of iron chelation Adults with transfusion-dependent thalassemia syndromes are living
therapy have extended the life span of patients with thalassemia longer into adulthood, with some approaching their seventh decade
major. 103,189,191,345 In a multicenter study of 1079 patients in Italy, the of life. It is likely in the coming decades that these patients will have
probability of survival to age 20 years was 96% for patients born improved life expectancies related to safer transfusion practices,
between 1975 and 1979, the time at which chelation therapy became improved screening of the blood supply, and better iron chelation
a regular part of the overall management of thalassemia major (Table medications. Therefore, the thalassemia patient born in the current
189
40.2). In contrast, the probabilities of survival at 20 years of age era may expect to spend the majority of their life as an adult.
were only 61% and 69% for those born in the periods of 1960 There is currently limited expertise among adult hematologists in
through 1964 and 1965 through 1969, respectively. Other investiga- the management of adult thalassemia patients. Transition plans are
tors have shown that survival or prevention of life-threatening com- essential for all pediatric patients as they enter adulthood, so that they
plications is strongly related to good chelation therapy, assessed either may receive age-appropriate care. Transition is especially important
by compliance or by control of iron stores (Fig. 40.11). 134,183,191 The in thalassemia, as they require the regular uninterrupted schedule of