
Page 696 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 696
588 Part V Red Blood Cells
Hb F:
O 2 Deoxygenation Hydroxyurea, decitabine?,
HDAC inhibitor?
Avoid Hb polymerization
dehydration Hb S concentration Replace Hb S with Hb A:
Exchange transfusion,
Acidosis Stem cell transplant
RBC rigidity RBC adhesion Hemolysis
Endothelial damage Anemia Nitric oxide
Erythropoietin? Antioxidants?
Iron chelation?
Coagulation Inflammatory
pathway activation pathway activation
Aspirin?
Vasoocclusion
Splenic, cerebral, pulmonary, renal, Renal, cardiac, Pulmonary
muscle, bone, retinal, skin complications skin complications hypertension
Vaccination, penicillin, vitamin supplementation,
analgesia, wound care, laser for retinopathy
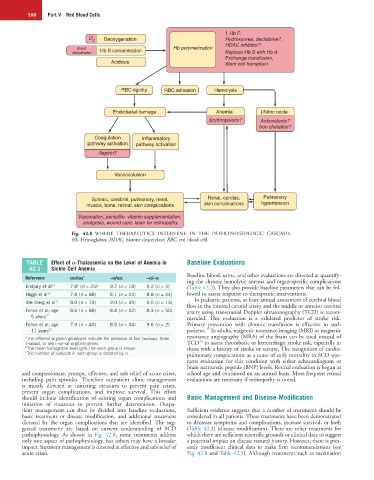
Fig. 42.8 WHERE THERAPEUTICS INTERVENE IN THE PATHOPHYSIOLOGIC CASCADE.
Hb, Hemoglobin; HDAC, histone deacetylase; RBC, red blood cell.
TABLE Effect of α-Thalassemia on the Level of Anemia in Baseline Evaluations
42.1 Sickle Cell Anemia
Reference αα/αα a −α/αα −α/−α Baseline blood, urine, and other evaluations are directed at quantify-
ing the chronic hemolytic anemia and organ-specific complications
Embury et al 29 7.8 (n = 25) c 9.7 (n = 18) 9.2 (n = 4) (Table 42.2). They also provide baseline parameters that can be fol-
b
Higgs et al 30 7.8 (n = 88) 8.1 (n = 44) 8.8 (n = 44) lowed to assess response to therapeutic interventions.
In pediatric patients, at least annual assessment of cerebral blood
Steinberg et al 31 8.0 (n = 73) 9.0 (n = 39) 9.5 (n = 13)
flow in the internal carotid artery and the middle or anterior cerebral
Felice et al; age 8.6 (n = 88) 8.4 (n = 52) 8.3 (n = 50) artery using transcranial Doppler ultrasonography (TCD) is recom-
5 years 32 mended. This evaluation is a validated predictor of stroke risk.
Felice et al; age 7.9 (n = 40) 8.5 (n = 34) 9.6 (n = 2) Primary prevention with chronic transfusion is effective in such
33
11 years 32 patients. In adults, magnetic resonance imaging (MRI) or magnetic
a The different α-globin genotypes indicate the presence of four (αα/αα), three resonance angiography (MRA) of the brain can be used instead of
34
(−α/αα), or two (−α/−α) α-globin genes. TCD to assess thrombotic or hemorrhagic stroke risk, especially in
b The mean hemoglobin level (g/dL) for each group is shown. those with a history of stroke or seizure. The recognition of cardio-
c The number of subjects in each group is denoted by n. pulmonary complications as a cause of early mortality in SCD war-
rants evaluation for this condition with either echocardiogram or
brain natriuretic peptide (BNP) levels. Retinal evaluation is begun at
and compassionate, prompt, effective, and safe relief of acute crises, school age and continued on an annual basis. More frequent retinal
including pain episodes. Therefore outpatient clinic management evaluations are necessary if retinopathy is noted.
is mostly directed at initiating measures to prevent pain crises,
prevent organ complications, and improve survival. This effort
should include identification of existing organ complications and Basic Management and Disease Modification
initiation of measures to prevent further deterioration. Outpa-
tient management can thus be divided into baseline evaluations, Sufficient evidence suggests that a number of treatments should be
basic treatment or disease modification, and additional treatment considered in all patients. These treatments have been demonstrated
dictated by the organ complications that are identified. The sug- to decrease symptoms and complications, increase survival, or both
gested treatments are based on current understanding of SCD (Table 42.3) (disease modification). There are other treatments for
pathophysiology. As shown in Fig. 42.8, some treatments address which there are sufficient scientific grounds or clinical data to suggest
only one aspect of pathophysiology, but others may have a broader a potential impact on disease natural history. However, there is pres-
impact. Inpatient management is directed at effective and safe relief of ently insufficient clinical data to make firm recommendations (see
acute crises. Fig. 42.8 and Table 42.3). Although treatments such as vaccination