
Page 707 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 707
Chapter 42 Sickle Cell Disease 599
internal carotid artery or middle cerebral artery, the stroke risk is in 1.0
excess of 10% per year (although this is still much lower than the risk
of recurrent stroke in a sickle cell patient after a first event, which is
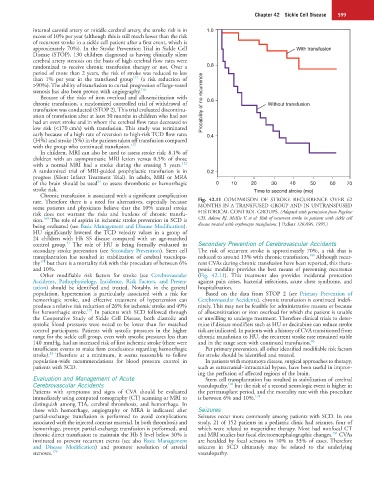
approximately 70%). In the Stroke Prevention Trial in Sickle Cell With transfusion
Disease (STOP), 130 children diagnosed as having clinically silent
cerebral artery stenosis on the basis of high cerebral flow rates were
randomized to receive chronic transfusion therapy or not. Over a 0.8
period of more than 2 years, the risk of stroke was reduced to less
171
than 1% per year in the transfused group (a risk reduction of
>90%). The ability of transfusion to curtail progression of large-vessel
stenosis has also been proven with angiography. 176
Because of the risks of iron overload and allosensitization with
chronic transfusion, a randomized controlled trial of withdrawal of Probability of no recurrence 0.6 Without transfusion
transfusion was conducted (STOP 2). This trial evaluated discontinu-
ation of transfusion after at least 30 months in children who had not
had an overt stroke and in whom the cerebral flow rates decreased to
low risk (<170 cm/s) with transfusion. This study was terminated
early because of a high rate of reversion to high-risk TCD flow rates 0.4
(34%) and stroke (5%) in the patients taken off transfusion compared
with the group who continued transfusion. 177
In children, MRI can also be used to assess stroke risk: 8.1% of
children with an asymptomatic MRI lesion versus 0.5% of those
172
with a normal MRI had a stroke during the ensuing 5 years.
A randomized trial of MRI-guided prophylactic transfusion is in 0.2
progress (Silent Infarct Treatment Trial). In adults, MRI or MRA
34
of the brain should be used to assess thrombotic or hemorrhagic 0 10 20 30 40 50 60 70
stroke risk. Time to second stroke (mo)
Chronic transfusion is associated with a significant complication
rate. Therefore there is a need for alternatives, especially because Fig. 42.11 COMPARISON OF STROKE RECURRENCE OVER 62
some patients and physicians believe that the 10% annual stroke MONTHS IN A TRANSFUSED GROUP AND IN UNTRANSFUSED
risk does not warrant the risks and burdens of chronic transfu- HISTORICAL CONTROL GROUPS. (Adapted with permission from Pegelow
160
sion. The role of aspirin in ischemic stroke prevention in SCD is CH, Adams RJ, McKie V, et al: Risk of recurrent stroke in patients with sickle cell
being evaluated (see Basic Management and Disease Modification). disease treated with erythrocyte transfusions. J Pediatr 126:896, 1995.)
HU significantly lowered the TCD velocity values in a group of
24 children with Hb SS disease compared with an age-matched
51
control group. The role of HU is being formally evaluated in Secondary Prevention of Cerebrovascular Accidents
secondary stroke prevention (see Secondary Prevention). Stem cell The risk of recurrent stroke is approximately 70%, a risk that is
180
transplantation has resulted in stabilization of cerebral vasculopa- reduced to around 13% with chronic transfusion. Although recur-
178
thy but there is a mortality risk with this procedure of between 6% rent CVAs during chronic transfusion have been reported, this thera-
and 10%. peutic modality provides the best means of preventing recurrence
Other modifiable risk factors for stroke (see Cerebrovascular (Fig. 42.11). This treatment also provides incidental protection
Accidents, Pathophysiology, Incidence, Risk Factors, and Presen- against pain crises, bacterial infections, acute chest syndrome, and
tation) should be identified and treated. Notably, in the general hospitalization.
population, hypertension is particularly associated with a risk for Based on the data from STOP 2 (see Primary Prevention of
hemorrhagic stroke, and effective treatment of hypertension can Cerebrovascular Accidents), chronic transfusion is continued indefi-
produce a relative risk reduction of 26% for ischemic stroke and 49% nitely. This may not be feasible for administrative reasons or because
179
for hemorrhagic stroke. In patients with SCD followed through of allosensitization or iron overload for which the patient is unable
the Cooperative Study of Sickle Cell Disease, both diastolic and or unwilling to undergo treatment. Therefore clinical trials to deter-
systolic blood pressures were noted to be lower than for matched mine if disease modifiers such as HU or decitabine can reduce stroke
control participants. Patients with systolic pressures in the higher risk are indicated. In patients with a history of CVA transitioned from
range for the sickle cell group, even with systolic pressures less than chronic transfusion to HU, the recurrent stroke rate remained stable
140 mmHg, had an increased risk of first ischemic stroke (there were and in the range seen with continued transfusion. 86
insufficient events to make firm conclusions regarding hemorrhagic Per primary prevention, all other identified modifiable risk factors
23
stroke). Therefore at a minimum, it seems reasonable to follow for stroke should be identified and treated.
population-wide recommendations for blood pressure control in In patients with moyamoya disease, surgical approaches to therapy,
patients with SCD. such as extracranial–intracranial bypass, have been useful in improv-
ing the perfusion of affected regions of the brain.
Evaluation and Management of Acute Stem cell transplantation has resulted in stabilization of cerebral
Cerebrovascular Accidents vasculopathy, but the risk of a second neurologic event is higher in
178
Patients with symptoms and signs of CVA should be evaluated the peritransplant period, and the mortality rate with this procedure
immediately using computed tomography (CT) scanning or MRI to is between 6% and 10%. 178
distinguish among TIA, cerebral thrombosis, and hemorrhage. In
those with hemorrhage, angiography or MRA is indicated after Seizures
partial-exchange transfusion is performed to avoid complications Seizures occur more commonly among patients with SCD. In one
associated with the injected contrast material. In both thrombosis and study, 21 of 152 patients in a pediatric clinic had seizures, four of
hemorrhage, prompt partial-exchange transfusion is performed, and which were related to meperidine therapy. Most had nonfocal CT
181
chronic direct transfusion to maintain the Hb S level below 30% is and MRI studies but focal electroencephalographic changes. CVAs
instituted to prevent recurrent events (see also Basic Management are heralded by focal seizures in 10% to 33% of cases. Therefore
and Disease Modification) and promote resolution of arterial seizures in SCD ultimately may be related to the underlying
stenoses. 176 vasculopathy.