
Page 968 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 968
Chapter 57 Pharmacology and Molecular Mechanisms of Antineoplastic Agents for Hematologic Malignancies 851
considerations in early phase I development. Numerous consider- registered at clinicaltrials.gov and all should have public reporting of
ations have guided dose-escalation strategies that accompany phase results.
I trial development. The starting dose is typically 10% of the lethal
dose in animals adjusted for species dose equivalency. In classic phase
I development, a modified Fibonacci dose schedule is used. Groups TRADITIONAL CYTOTOXIC ANTINEOPLASTIC AGENTS
of three patients are treated at each of the following doses until the TARGETING THE CELL CYCLE AND DNA
maximum tolerated dose is observed: 1N (the starting dose), 2N,
5N, 7N, 9N, 12N, and 16N. Typically, the maximum tolerated Targeting Tumor Cell Growth Kinetics
dose is defined as the maximum dose not causing irreversible toxicity
of any type and causing less than grade 4 toxicity in any organ. Malignant hematopoietic cells proliferate more and differentiate less
Newer agents often have off-target toxicities, and these complicate than their normal counterparts. The cell cycle consists of a series of
drug evaluation because the dose-dependent toxicities are replaced stages through which normal and neoplastic cells proceed during the
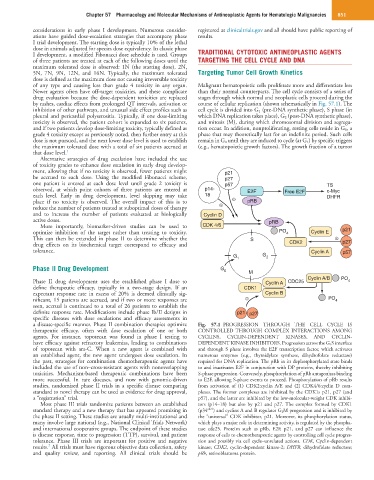
by rashes, cardiac effects from prolonged QT intervals, activation or course of cellular replication (shown schematically in Fig. 57.1). The
inhibition of other pathways, and unusual side effect profiles such as cell cycle is divided into G 1 (pre-DNA synthetic phase), S phase (in
pleural and pericardial polyserositis. Typically, if one dose-limiting which DNA replication takes place), G 2 (post-DNA synthetic phase),
toxicity is observed, the patient cohort is expanded to six patients, and mitosis (M), during which chromosomal division and segrega-
and if two patients develop dose-limiting toxicity, typically defined as tion occur. In addition, nonproliferating, resting cells reside in G 0, a
grade 4 toxicity except as previously noted, then further entry at this phase that may theoretically last for an indefinite period. Such cells
dose is not pursued, and the next lower dose level is used to establish remain in G 0 until they are induced to cycle (at G 1) by specific triggers
the maximum tolerated dose with a total of six patients accrued at (e.g., hematopoietic growth factors). The growth fraction of a tumor
that dose level. 1
Alternative strategies of drug escalation have included the use
of toxicity grades to enhance dose escalation in early drug develop-
ment, allowing that if no toxicity is observed, fewer patients might p21
be accrued to each dose. Using the modified Fibonacci scheme, p27
one patient is entered at each dose level until grade 2 toxicity is p57 TS
observed, at which point cohorts of three patients are entered at p14- E2F Free E2F c-Myc
each level. Early in drug development, level skipping may take 18 DHFR
place if no toxicity is observed. The overall impact of this is to - pRB
reduce the number of patients treated at suboptimal doses of therapy -
and to increase the number of patients evaluated at biologically Cyclin D
active doses. pRB
More importantly, biomarker-driven studies can be used to CDK 4/6
optimize inhibition of the target rather than treating to toxicity. PO 4 Cyclin E p21
This can then be extended in phase II to determine whether the S -
drug effects on its biochemical target correspond to efficacy and CDK2 p27
tolerance. Cyclin A p57
G 1 G 2
Phase II Drug Development G 0 M
Cyclin A/B PO
Phase II drug development uses the established phase I dose to Cyclin A CDC25 4
define therapeutic efficacy, typically in a two-stage design. If an CDK1
expectant response rate in excess of 20% is deemed clinically sig- Cyclin B
nificant, 15 patients are accrued, and if two or more responses are - PO 4
seen, accrual is continued to a total of 26 patients to establish the
definite response rate. Modifications include phase Ib/II designs in p21 p27
specific diseases with dose escalations and efficacy assessments in
a disease-specific manner. Phase II combination therapies optimize Fig. 57.1 PROGRESSION THROUGH THE CELL CYCLE IS
therapeutic efficacy, often with dose escalation of one or both CONTROLLED THROUGH COMPLEX INTERACTIONS AMONG
agents. For instance, topotecan was found in phase I testing to CYCLINS, CYCLIN-DEPENDENT KINASES, AND CYCLIN-
have efficacy against refractory leukemias, leading to combinations DEPENDENT KINASE INHIBITORS. Progression across the G 1 S interface
of topotecan with ara-C. When a new agent is combined with and through S phase involves the E2F transcription factor, which activates
an established agent, the new agent undergoes dose escalation. In numerous enzymes (e.g., thymidylate synthase, dihydrofolate reductase)
the past, strategies for combination chemotherapeutic agents have required for DNA replication. The pRb in its dephosphorylated state binds
included the use of non–cross-resistant agents with nonoverlapping to and inactivates E2F in conjunction with DP proteins, thereby inhibiting
toxicities. Mechanism-based therapeutic combinations have been S-phase progression. Conversely, phosphorylation of pRb antagonizes binding
more successful. In rare diseases, and now with genomic-driven to E2F, allowing S-phase events to proceed. Phosphorylation of pRb results
studies, randomized phase II trials in a specific disease comparing from activation of (1) CDK2:cyclin A/E and (2) CDK4/6:cyclin D com-
standard to novel therapy can be used as evidence for drug approval, plexes. The former complexes are inhibited by the CDK1s p21, p27 (and
a “registration” trial. p57), and the latter are inhibited by the low-molecular-weight CDK inhibi-
Most phase III trials randomize patients between an established tors (p14–18) but also by p21 and p27. The complex formed by CDK1
standard therapy and a new therapy that has appeared promising in (p34 cdc2 ) and cyclins A and B regulates G 2 M progression and is inhibited by
the phase II setting. These studies are usually multi-institutional and the “universal” CDK inhibitor, p21. Moreover, its phosphorylation status,
many involve large national (e.g., National Clinical Trials Network) which plays a major role in determining activity, is regulated by the phospha-
and international cooperative groups. The endpoint of these studies tase cdc25. Proteins such as pRb, E2F, p21, and p27 can influence the
is disease response, time to progression (TTP), survival, and patient response of cells to chemotherapeutic agents by controlling cell cycle progres-
tolerance. Phase III trials are important for positive and negative sion and possibly via cell cycle–unrelated actions. CDK, Cyclin-dependent
2
results. All trials must have rigorous objective data collection, safety kinase; CDK2, cyclin-dependent kinase-2; DHFR, dihydrofolate reductase;
and quality review, and reporting. All clinical trials should be pRb, retinoblastoma protein.