
Page 133 - Williams Hematology ( PDFDrive )
P. 133
108 Part III: Epochal Hematology Chapter 7: Hematology of the Fetus and Newborn 109
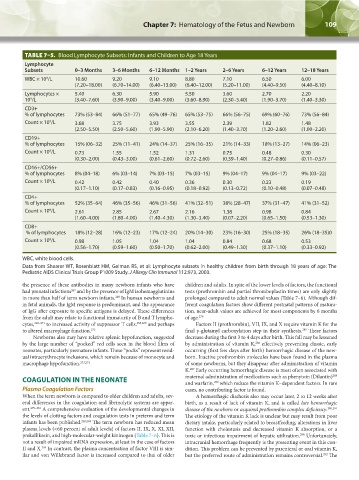
TABLE 7–5. Blood Lymphocyte Subsets: Infants and Children to Age 18 Years
Lymphocyte
Subsets 0–3 Months 3–6 Months 6–12 Months 1–2 Years 2–6 Years 6–12 Years 12–18 Years
WBC × 10 /L 10.60 9.20 9.10 8.80 7.10 6.50 6.00
9
(7.20–18.00) (6.70–14.00) (6.40–13.00) (6.40–12.00) (5.20–11.00) (4.40–9.50) (4.40–8.10)
Lymphocytes × 5.40 6.30 5.90 5.50 3.60 2.70 2.20
10 /L (3.40–7.60) (3.90–9.00) (3.40–9.00) (3.60–8.90) (2.30–5.40) (1.90–3.70) (1.40–3.30)
9
CD3+
% of lymphocytes 73% (53–84) 66% (51–77) 65% (49–76) 65% (53–75) 66% (56–75) 69% (60–76) 73% (56–84)
Count × 10 /L 3.68 3.75 3.93 3.55 2.39 1.82 1.48
9
(2.50–5.50) (2.50–5.60) (1.90–5.90) (2.10–6.20) (1.40–3.70) (1.20–2.60) (1.00–2.20)
CD19+
% of lymphocytes 15% (06–32) 25% (11–41) 24% (14–37) 25% (16–35) 21% (14–33) 18% (13–27) 14% (06–23)
Count × 10 /L 0.73 1.55 1.52 1.31 0.75 0.48 0.30
9
(0.30–2.00) (0.43–3.00) (0.61–2.60) (0.72–2.60) (0.39–1.40) (0.27–0.86) (0.11–0.57)
CD16+/CD56+
% of lymphocytes 8% (04–18) 6% (03–14) 7% (03–15) 7% (03–15) 9% (04–17) 9% (04–17) 9% (03–22)
Count × 10 /L 0.42 0.42 0.40 0.36 0.30 0.23 0.19
9
(0.17–1.10) (0.17–0.83) (0.16–0.95) (0.18–0.92) (0.13–0.72) (0.10–0.48) (0.07–0.48)
CD4+
% of lymphocytes 52% (35–64) 46% (35–56) 46% (31–56) 41% (32–51) 38% (28–47) 37% (31–47) 41% (31–52)
Count × 10 /L 2.61 2.85 2.67 2.16 1.38 0.98 0.84
9
(1.60–4.00) (1.80–4.00) (1.40–4.30) (1.30–3.40) (0.07–2.20) (0.65–1.50) (0.53–1.30)
CD8+
% of lymphocytes 18% (12–28) 16% (12–23) 17% (12–24) 20% (14–30) 23% (16–30) 25% (18–35) 26% (18–35)0
Count × 10 /L 0.98 1.05 1.04 1.04 0.84 0.68 0.53
9
(0.56–1.70) (0.59–1.60) (0.50–1.70) (0.62–2.00) (0.49–1.30) (0.37–1.10) (0.33–0.92)
WBC, white blood cells.
Data from Shearer WT, Rosenblatt HM, Gelman RS, et al: Lymphocyte subsets in healthy children from birth through 18 years of age: The
Pediatric AIDS Clinical Trials Group P1009 Study. J Allergy Clin Immunol 112:973, 2003.
the presence of these antibodies in many newborn infants who have children and adults. In spite of the lower levels of factors, the functional
had prenatal infections and by the presence of IgM isohemagglutinins tests (prothrombin and partial thromboplastin times) are only slightly
267
in more than half of term newborn infants. In human newborns and prolonged compared to adult normal values (Table 7–6). Although dif-
268
in fetal animals, the IgM response is predominant, and the appearance ferent coagulation factors show different postnatal patterns of matura-
of IgG after exposure to specific antigens is delayed. These differences tion, near-adult values are achieved for most components by 6 months
from the adult may relate to functional immaturity of B and T lympho- of age. 278
cytes, 269–271 to increased activity of suppressor T cells, 258,269 and perhaps Factors II (prothrombin), VII, IX, and X require vitamin K for the
to altered macrophage function. 272 final γ-glutamyl carboxylation step in their synthesis. These factors
285
Newborns also may have relative splenic hypofunction, suggested decrease during the first 3 to 4 days after birth. This fall may be lessened
by the large number of “pocked” red cells seen in the blood films of by administration of vitamin K, effectively preventing classic, early
286
neonates, particularly premature infants. These “pocks” represent resid- occurring (first few days after birth) hemorrhagic disease of the new-
ual intraerythrocyte inclusions, which remain because of monocyte and born. Inactive prothrombin molecules have been found in the plasma
macrophage hypofunction. 273,274 of some newborns, but they disappear after administration of vitamin
K. Early occurring hemorrhagic disease is most often associated with
287
288
COAGULATION IN THE NEONATE maternal administration of medications such as phenytoin (Dilantin)
and warfarin, which reduce the vitamin K–dependent factors. In rare
289
Plasma Coagulation Factors cases, no contributing factor is found.
When the term newborn is compared to older children and adults, sev- A hemorrhagic diathesis also may occur later, 2 to 12 weeks after
eral differences in the coagulation and fibrinolytic systems are appar- birth, as a result of lack of vitamin K, and is called late hemorrhagic
ent. 275–281 A comprehensive evaluation of the developmental changes in disease of the newborn or acquired prothrombin complex deficiency. 290,291
the levels of clotting factors and coagulation tests in preterm and term The etiology of the vitamin K lack is unclear but may result from poor
infants has been published. 282,283 The term newborn has reduced mean dietary intake, particularly related to breastfeeding, alterations in liver
plasma levels (<60 percent of adult levels) of factors II, IX, X, XI, XII, function with cholestasis and decreased vitamin K absorption, or a
prekallikrein, and high-molecular-weight kininogen (Table 7–6). This is toxic or infectious impairment of hepatic utilization. Unfortunately,
290
not a result of impaired mRNA expression, at least in the case of factors intracranial hemorrhage frequently is the presenting event in this con-
284
II and X. In contrast, the plasma concentration of factor VIII is sim- dition. This problem can be prevented by parenteral or oral vitamin K,
ilar and von Willebrand factor is increased compared to that of older but the preferred route of administration remains controversial. The
292
Kaushansky_chapter 07_p0097-0118.indd 109 9/18/15 10:13 PM