
Page 765 - Williams Hematology ( PDFDrive )
P. 765
740 Part VI: The Erythrocyte Chapter 48: The Thalassemias: Disorders of Globin Synthesis 741
who also inherited α- or β-globin structural variants provide a clear
7,9
picture of the action of the thalassemia determinants. In homozygous
Excess β-thalassemia, β-globin synthesis is either absent or markedly reduced.
The result is excessive production of α-globin chains. α-Globin chains
Precipitation are incapable of forming a viable hemoglobin tetramer, so the chains
HgbF precipitate in red cell precursors. The resulting inclusion bodies can be
Selective survival of Hemolysis Destruction of RBC demonstrated by both light and electron microscopy. 169,170 In the mar-
HgbF-containing cells precursors row, precipitation can be seen in the earliest hemoglobinized precursors
171
and throughout the erythroid maturation pathway. These large inclu-
Splenomegaly Ineffective sions are responsible for intramedullary destruction of red cell precur-
(pooling, plasma erythropoiesis sors and hence for the ineffective erythropoiesis characterizing all the
volume β-thalassemias. A large proportion of the developing erythroblasts are
expansion)
destroyed within the marrow in severe cases. Any red cells that are
172
released are prematurely destroyed by mechanisms that are considered
High oxygen Anemia
affinity of red cells below in “Mechanisms and Consequences of Erythroid Precursor and
Red Cell Damage.” β-Thalassemia heterozygotes also have imbalanced
Tissue hypoxia globin-chain synthesis, but the magnitude of α-chain excess is much
less and presumably can be resolved by the proteolytic enzymes of the
Erythropoietin Transfusion
173
red cell precursors. Notwithstanding, a mild degree of ineffective ery-
thropoiesis occurs.
Marrow expansion
Although there is marked globin-chain imbalance in the severe
Increased iron α-thalassemias, 7,167 the excess γ and β chains form homotetramers that
absorption do not precipitate in the red cell precursors to the same extent as excess
Bone deformity α chains in β-thalassemia. Hence the pathophysiology of anemia is fun-
Increased metabolic rate
Wasting Iron loading damentally different between the two conditions.
Gout
Folate deficiency Endocrine deficiencies
Cirrhosis
Cardiac failure MECHANISMS AND CONSEQUENCES OF
Death ERYTHROID PRECURSOR AND RED CELL
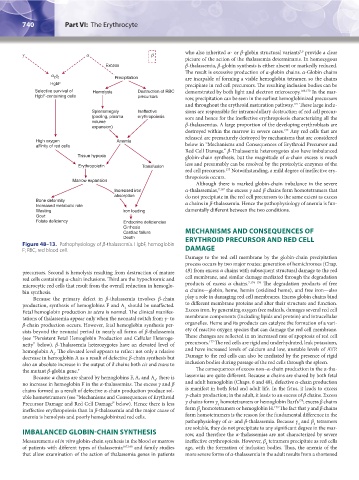
Figure 48–13. Pathophysiology of β-thalassemia. HgbF, hemoglobin
F; RBC, red blood cell. DAMAGE
Damage to the red cell membrane by the globin-chain precipitation
process occurs by two major routes: generation of hemichromes (Chap.
precursors. Second is hemolysis resulting from destruction of mature 49) from excess α chains with subsequent structural damage to the red
red cells containing α-chain inclusions. Third are the hypochromic and cell membrane, and similar damage mediated through the degradation
microcytic red cells that result from the overall reduction in hemoglo- products of excess α chains. 7,174–176 The degradation products of free
bin synthesis. α chains—globin, heme, hemin (oxidized heme), and free iron—also
Because the primary defect in β-thalassemia involves β-chain play a role in damaging red cell membranes. Excess globin chains bind
production, synthesis of hemoglobins F and A should be unaffected. to different membrane proteins and alter their structure and function.
2
Fetal hemoglobin production in utero is normal. The clinical manifes- Excess iron, by generating oxygen free radicals, damages several red cell
tations of thalassemia appear only when the neonatal switch from γ- to membrane components (including lipids and protein) and intracellular
β-chain production occurs. However, fetal hemoglobin synthesis per- organelles. Heme and its products can catalyze the formation of a vari-
sists beyond the neonatal period in nearly all forms of β-thalassemia ety of reactive oxygen species that can damage the red cell membrane.
(see “Persistent Fetal Hemoglobin Production and Cellular Heteroge- These changes are reflected in an increased rate of apoptosis of red cell
177
neity” below). β-Thalassemia heterozygotes have an elevated level of precursors. The red cells are rigid and underhydrated, leak potassium,
hemoglobin A . The elevated level appears to reflect not only a relative and have increased levels of calcium and low, unstable levels of ATP.
2
decrease in hemoglobin A as a result of defective β-chain synthesis but Damage to the red cells can also be mediated by the presence of rigid
also an absolute increase in the output of δ chains both cis and trans to inclusion bodies during passage of the red cells through the spleen.
the mutant β-globin gene. 7 The consequences of excess non–α-chain production in the α-tha-
Because α chains are shared by hemoglobins F, A, and A , there is lassemias are quite different. Because α chains are shared by both fetal
2
no increase in hemoglobin F in the α-thalassemias. The excess γ and β and adult hemoglobin (Chaps. 6 and 48), defective α-chain production
chains formed as a result of defective α-chain production produce sol- is manifest in both fetal and adult life. In the fetus, it leads to excess
uble homotetramers (see “Mechanisms and Consequences of Erythroid γ-chain production; in the adult, it leads to an excess of β chains. Excess
178
Precursor Damage and Red Cell Damage” below). Hence there is less γ chains form γ homotetramers or hemoglobin Bart’s ; excess β chains
4
179
ineffective erythropoiesis than in β-thalassemia and the major cause of form β homotetramers or hemoglobin H. The fact that γ and β chains
4
anemia is hemolysis and poorly hemoglobinized red cells. form homotetramers is the reason for the fundamental difference in the
pathophysiology of α- and β-thalassemia. Because γ and β tetramers
4
4
are soluble, they do not precipitate to any significant degree in the mar-
IMBALANCED GLOBIN-CHAIN SYNTHESIS row, and therefore the α-thalassemias are not characterized by severe
Measurements of in vitro globin-chain synthesis in the blood or marrow ineffective erythropoiesis. However, β tetramers precipitate as red cells
4
of patients with different types of thalassemia 167,168 and family studies age, with the formation of inclusion bodies. Thus, the anemia of the
that allow examination of the action of thalassemia genes in patients more severe forms of α-thalassemia in the adult results from a shortened
Kaushansky_chapter 48_p0725-0758.indd 740 9/18/15 2:57 PM