
Page 1032 - Clinical Immunology_ Principles and Practice ( PDFDrive )
P. 1032
CHaPter 74 Immunological Ocular Disease 995
TABLE 74.1 Diagnostic Categories
of Uveitis
Diagnostic Group Diagnosis
Infectious Viral Herpes simplex, Herpes zoster
causes Cytomegalovirus (CMV) infection
Chikungunya
Human T-lymphotropic virus 1
(HTLV-1) infection
Mumps
West Nile virus infection
Ebola
Zika virus infection
Bacterial or Atypical Mycobacterium infection
spirochetal Bacterial endocarditis
Bartonella infection
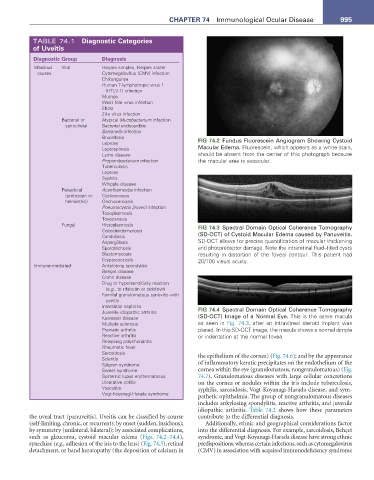
Brucellosis FIG 74.2 Fundus Fluorescein Angiogram Showing Cystoid
Leprosy
Leptospirosis Macular Edema. Fluorescein, which appears as a white stain,
Lyme disease should be absent from the center of this photograph because
Propionibacterium infection the macular area is avascular.
Tuberculosis
Leprosy
Syphilis
Whipple disease
Parasitical Acanthamoeba infection
(protozoan or Cysticercosis
helminthic) Onchocerciasis
Pneumocystis jiroveci infection
Toxoplasmosis
Toxocariasis
Fungal Histoplasmosis FIG 74.3 Spectral Domain Optical Coherence Tomography
Coccidioidomycosis
Candidiasis (SD-OCT) of Cystoid Macular Edema caused by Panuveitis.
Aspergillosis SD-OCT allows for precise quantification of macular thickening
Sporotrichosis and photoreceptor damage. Note the intraretinal fluid–filled cysts
Blastomycosis resulting in distortion of the foveal contour. This patient had
Cryptococcosis 20/100 visual acuity.
Immune-mediated Ankylosing spondylitis
Behçet disease
Crohn disease
Drug or hypersensitivity reaction
(e.g., to rifabutin or cidofovir)
Familial granulomatous synovitis with
uveitis
Interstitial nephritis FIG 74.4 Spectral Domain Optical Coherence Tomography
Juvenile idiopathic arthritis
Kawasaki disease (SD-OCT) Image of a Normal Eye. This is the same macula
Multiple sclerosis as seen in Fig. 74.3, after an intravitreal steroid implant was
Psoriatic arthritis placed. In this SD-OCT image, the macula shows a normal dimple
Reactive arthritis or indentation at the normal fovea.
Relapsing polychondritis
Rheumatic fever
Sarcoidosis the epithelium of the cornea) (Fig. 74.6); and by the appearance
Scleritis
Sjögren syndrome of inflammatory keratic precipitates on the endothelium of the
Sweet syndrome cornea within the eye (granulomatous, nongranulomatous) (Fig.
Systemic lupus erythematosus 74.7). Granulomatous diseases with large cellular concretions
Ulcerative colitis on the cornea or nodules within the iris include tuberculosis,
Vasculitis syphilis, sarcoidosis, Vogt-Koyanagi-Harada disease, and sym-
Vogt-Koyanagi-Harada syndrome
pathetic ophthalmia. The group of nongranulomatous diseases
includes ankylosing spondylitis, reactive arthritis, and juvenile
idiopathic arthritis. Table 74.2 shows how these parameters
the uveal tract (panuveitis). Uveitis can be classified by course contribute to the differential diagnosis.
(self-limiting, chronic, or recurrent); by onset (sudden, insidious); Additionally, ethnic and geographical considerations factor
by symmetry (unilateral, bilateral); by associated complications, into the differential diagnosis. For example, sarcoidosis, Behçet
such as glaucoma, cystoid macular edema (Figs. 74.2–74.4), syndrome, and Vogt-Koyanagi-Harada disease have strong ethnic
synechiae (e.g., adhesion of the iris to the lens) (Fig. 74.5), retinal predispositions, whereas certain infections, such as cytomegalovirus
detachment, or band keratopathy (the deposition of calcium in (CMV) in association with acquired immunodeficiency syndrome