
Page 1532 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1532
CHAPTER 110: Special Considerations in the Surgical Patient 1051
+20
0
% Change VC –20
–40
Superficial (spinal)
Superficial (gen)
–60
Thoracotomy
Lower abdominal
Posterior
Upper abdominal
–80
Preop 0 1 2 3 5
Postoperative day
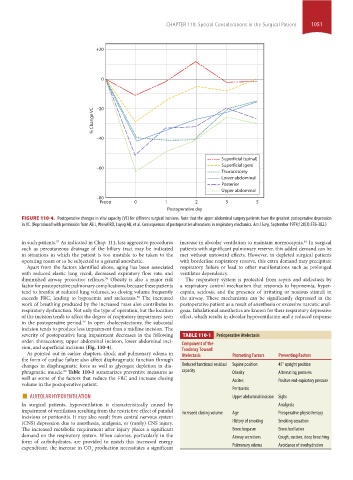
FIGURE 110-4. Postoperative changes in vital capacity (VC) for different surgical incisions. Note that the upper abdominal surgery patients have the greatest postoperative depression
in VC. (Reproduced with permission from Ali J, Weisel RD, Layug AB, et al. Consequences of postoperative alterations in respiratory mechanics. Am J Surg. September 1974;128(3):376-382.)
in such patients. As indicated in Chap. 111, less aggressive procedures increase in alveolar ventilation to maintain normocapnia. In surgical
57
61
such as percutaneous drainage of the biliary tract may be indicated patients with significant pulmonary reserve, this added demand can be
in situations in which the patient is too unstable to be taken to the met without untoward effects. However, in depleted surgical patients
operating room or to be subjected to a general anesthetic. with borderline respiratory reserve, this extra demand may precipitate
Apart from the factors identified above, aging has been associated respiratory failure or lead to other manifestations such as prolonged
with reduced elastic lung recoil, decreased expiratory flow rate, and ventilator dependency.
diminished airway protective reflexes. Obesity is also a major risk The respiratory system is protected from sepsis and atelectasis by
38
factor for postoperative pulmonary complications, because these patients a respiratory control mechanism that responds to hypoxemia, hyper-
tend to breathe at reduced lung volumes, so closing volume frequently capnia, acidosis, and the presence of irritating or noxious stimuli in
exceeds FRC, leading to hypoxemia and atelectasis. The increased the airway. These mechanisms can be significantly depressed in the
58
work of breathing produced by the increased mass also contributes to postoperative patient as a result of anesthesia or excessive narcotic anal-
respiratory dysfunction. Not only the type of operation, but the location gesia. Inhalational anesthetics are known for their respiratory depressive
of the incision tends to affect the degree of respiratory impairment seen effect, which results in alveolar hypoventilation and a reduced response
in the postoperative period. In open cholecystectomy, the subcostal
59
incision tends to produce less impairment than a midline incision. The
severity of postoperative lung impairment decreases in the following TABLE 110-1 Perioperative Atelectasis
order: thoracotomy, upper abdominal incision, lower abdominal inci- Component of the
sion, and superficial incisions (Fig. 110-4). Tendency Toward
As pointed out in earlier chapters, shock and pulmonary edema in Atelectasis Promoting Factors Preventing Factors
the form of cardiac failure also affect diaphragmatic function through
changes in diaphragmatic force as well as glycogen depletion in dia- Reduced functional residual Supine position 45° upright position
phragmatic muscle. Table 110-1 summarizes preventive measures as capacity Obesity Alternating postures
60
well as some of the factors that reduce the FRC and increase closing Ascites Positive end-expiratory pressure
volume in the postoperative patient. Peritonitis
■ ALVEOLAR HYPOVENTILATION Upper abdominal incision Sighs
In surgical patients, hypoventilation is characteristically caused by Analgesia
impairment of ventilation resulting from the restrictive effect of painful Increased closing volume Age Preoperative physiotherapy
incisions or peritonitis. It may also result from central nervous system
(CNS) depression due to anesthesia, analgesia, or (rarely) CNS injury. History of smoking Smoking cessation
The increased metabolic requirement after injury places a significant Bronchospasm Bronchodilation
demand on the respiratory system. When calories, particularly in the Airway secretions Cough, suction, deep breathing
form of carbohydrates, are provided to match this increased energy
expenditure, the increase in CO production necessitates a significant Pulmonary edema Avoidance of overhydration
2
section10.indd 1051 1/20/2015 9:19:31 AM