
Page 1549 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1549
1068 PART 10: The Surgical Patient
pleural cavities, and electrical anatomy of the heart are mandatory in pneumothoraces. For example, when there is no communication
order to be able to recognize when complications occur and how they between the cavities, postoperative effusions are likely to be transudative
may be a technical or functional complication of the surgery. and can be managed medically rather than with a pleural tap or drain
The coronary vessels are widely described as three main arteries, that would be required for a bloody postoperative effusion.
although there are only two ostia (origins) that come directly off the
aorta. There are three sinuses of Valsalva that protrude just above the ■ BASIC OPERATIVE TERMINOLOGY
aortic valve to the level of the sinotubular junction (STJ). The left coro-
nary sinus is located on the left of the aorta and gives off the left main Cardiac operations can be performed in a variety of ways. Off-pump,
(LM) artery. The right coronary sinus is located anteriorly and gives off cross-clamp time, and circ arrest can be anxiety-producing terms to indi-
the right coronary artery (RCA). This anatomic location is important viduals who have never been in a cardiac case. Again, understanding
to understanding why the right heart is at risk for air embolism as the the importance of these terms is vital to understanding postoperative
right coronary artery is the first anterior branch off of the aorta. The management of cardiac patients. Cardiopulmonary bypass, CPB, and
noncoronary sinus has no vessels arising from it. The left main artery on-pump are terms used to describe the process by which the heart
further divides into the left anterior descending (LAD) artery and the and lungs are literally bypassed from their typical blood flow. Venous
left circumflex artery (LCx). Occasionally, a third vessel comes directly drainage occurs from the right atrium or vena cava into the bypass
off the left main called the ramus intermedius (RI). The LAD branches machine and then is redelivered to the arterial system with a managed
into septal perforators that feed the septum and the diagonal vessels flow system after oxygenating and decarboxylating. CPB is most often
that along with the LAD and RI, if present, feed the anterior heart. The performed in the chest cavity utilizing the right atrium and aorta, but
terminal LAD feeds the apex of the left ventricle. The LCx is so named can be performed in the groin or axilla as well. Bypass is associated
since it encircles the heart in a posterior fashion. It gives off obtuse mar- with a systemic inflammatory response. The longer the bypass run,
ginal branches that are important to the blood supply of the lateral heart the greater the response; it can affect every organ, for example, hepatic
and occasionally the posterior descending artery (PDA) that supplies the insufficiency, renal insufficiency, hypocoagulability, vasodilation. This
mitral valve. The primary branches of the RCA that are bypassed include is why patients who undergo bypass procedures typically require vaso-
the posterolateral (RPL) branch feeding the inferior heart and the PDA pressors and fluid administration in the first 24 to 36 hours after a
that supplies the posterior heart and septum. In the majority of the cardiac procedure.
population, the PDA arises from the right coronary artery. The origin Cross-clamp, “XC”, refers to application of a clamp across the aorta to
of the PDA leads to a description of a heart being right, left, or codomi- occlude flow from the heart to the arterial system. Alternatively in mini-
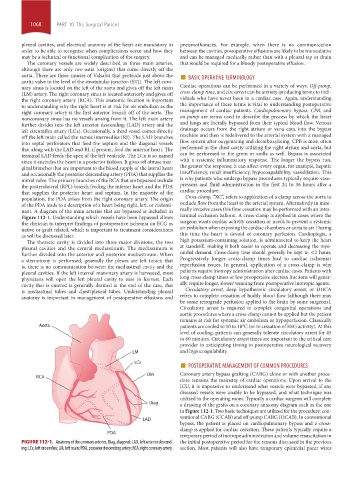
nant. A diagram of the main arteries that are bypassed is included in mally invasive cases this flow cessation may be performed with an intra-
Figure 112-1. Understanding which vessels have been bypassed allows luminal occlusion balloon. A cross-clamp is applied in cases where the
the clinician to interpret findings of postoperative ischemia on ECG as surgeon wants cardiac activity cessation or needs to prevent a systemic
native or graft related, which is important to treatment considerations air embolism when exposing the cardiac chambers or aorta to air. During
as will be discussed later. this time the heart is devoid of coronary perfusion. Cardioplegia, a
The thoracic cavity is divided into three major divisions, the two high potassium-containing solution, is administered to keep the heart
pleural cavities and the central mediastinum. The mediastinum is at standstill, making it both easier to operate and decreasing the myo-
further divided into the anterior and posterior mediastinum. When cardial demand. Cross-clamp time should generally be kept to <2 hours.
a sternotomy is performed, generally the pleura are left intact; that Progressively longer cross-clamp times lead to cardiac ischemia/
is, there is no communication between the mediastinal cavity and the reperfusion issues. In general, application of a cross-clamp is why
pleural cavities. If the left internal mammary artery is harvested, most patients require inotropy administration after cardiac cases. Patients with
physicians will open the left pleural cavity to ease in harvest. Each long cross-clamp times or low preoperative ejection fractions will gener-
cavity that is entered is generally drained at the end of the case, that ally require longer, slower weaning from postoperative inotropic agents.
is mediastinal tubes and chest/pleural tubes. Understanding pleural Circulatory arrest, deep hypothermic circulatory arrest, or DHCA
anatomy is important in management of postoperative effusions and refers to complete cessation of bodily blood flow (although there may
be some retrograde perfusion applied to the brain by some surgeons).
Circulatory arrest is required in complex congenital operations and
aortic procedures where a cross-clamp cannot be applied but the patient
remains at risk for systemic air embolism or hypoperfusion. Classically
Aorta patients are cooled to 10 to 18°C (or to cessation of EEG activity). At this
level of cooling, patients can generally tolerate circulatory arrest for 45
to 60 minutes. Circulatory arrest times are important to the critical care
provider in anticipating timing to postoperative neurological recovery
LM and hypocoagulability.
■
LCx POSTOPERATIVE MANAGEMENT OF COMMON PROCEDURES
OM Coronary artery bypass grafting (CABG) alone or with another proce-
RCA
dure remains the mainstay of cardiac operations. Upon arrival to the
ICU, it is imperative to understand what vessels were bypassed, if any
diseased vessels were unable to be bypassed, and what technique was
utilized in the operating room. Typically a cardiac surgeon will complete
Diag a drawing of the grafts on a coronary anatomy diagram such as the one
in Figure 112-1. Two basic techniques are utilized for the procedure: con-
ventional CABG (CCAB) and off-pump CABG (OCAB). In conventional
LAD
bypass, the patient is placed on cardiopulmonary bypass and a cross-
clamp is applied for cardiac cessation. These patients typically require a
PDA
temporary period of inotrope administration and volume resuscitation in
FIGURE 112-1. Anatomy of the coronary arteries. Diag, diagonal; LAD, left anterior descend- the initial postoperative period for the reasons discussed in the previous
ing; LCx, left circumflex; LM, left main; PDA, posterior descending artery; RCA, right coronary artery. section. Most patients will also have temporary epicardial pacer wires
section10.indd 1068 1/20/2015 9:19:43 AM