
Page 1604 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1604
CHAPTER 118: Head Injury 1123
FIGURE 118-4. Head CT demonstrating a left frontotemporoparietal acute subdural
hematoma with mass effect and mild midline shift. Subdural hematomas do not respect
suture lines and are typically crescent shaped.
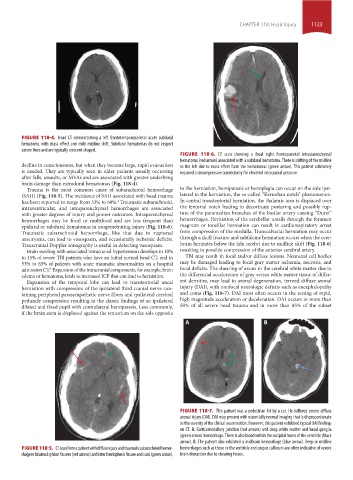
FIGURE 118-6. CT scan showing a focal right frontoparietal intraparenchymal
hematoma (red arrow) associated with a subdural hematoma. There is shifting of the midline
decline in consciousness, but when they become large, rapid evacuation to the left due to mass effect from the hematomas (green arrow). This patient ultimately
is needed. They are typically seen in older patients usually occurring required a decompressive craniectomy for elevated intracranial pressure.
after falls, assaults, or MVAs and are associated with greater underlying
brain damage than extradural hematomas (Fig. 118-4).
Trauma is the most common cause of subarachnoid hemorrhage to the herniation, hemiparesis or hemiplegia can occur on the side ipsi-
(SAH) (Fig. 118-5). The incidence of SAH associated with head trauma lateral to the herniation, the so-called “Kernohan notch” phenomenon.
has been reported to range from 33% to 60%. Traumatic subarachnoid, In central transtentorial herniation, the thalamic area is displaced over
4
intraventricular, and intraparenchymal hemorrhages are associated the tentorial notch leading to decorticate posturing and possibly rup-
with greater degrees of injury and poorer outcomes. Intraparenchymal ture of the paramedian branches of the basilar artery causing “Duret”
hemorrhages may be focal or multifocal and are less frequent than hemorrhages. Herniation of the cerebellar tonsils through the foramen
epidural or subdural hematomas in nonpenetrating injury (Fig. 118-6). magnum or tonsillar herniation can result in cardiorespiratory arrest
Traumatic subarachnoid hemorrhage, like that due to ruptured from compression of the medulla. Transcalvarial herniation may occur
aneurysms, can lead to vasospasm, and occasionally ischemic deficits. through a skull fracture and subfalcine herniation occurs when the cere-
Transcranial Doppler sonography is useful in detecting vasospasm. brum herniates below the falx cerebri due to midline shift (Fig. 118-6)
Brain swelling with associated intracranial hypertension develops in 10% resulting in possible compression of the anterior cerebral artery.
to 15% of severe TBI patients who have an initial normal head CT, and in TBI may result in focal and/or diffuse lesions. Neuronal cell bodies
53% to 63% of patients with acute traumatic abnormalities on a hospital may be damaged leading to focal gray matter ischemia, necrosis, and
admission CT. Expansion of the intracranial components, for example, brain focal deficits. The shearing of axons in the cerebral white matter due to
5
edema or hematoma, leads to increased ICP that can lead to herniation. the differential acceleration of gray versus white matter tissue of differ-
Expansion of the temporal lobe can lead to transtentorial uncal ent densities, may lead to axonal degeneration, termed diffuse axonal
herniation with compression of the ipsilateral third cranial nerve con- injury (DAI), with nonfocal neurologic deficits such as encephalopathy
taining peripheral parasympathetic nerve fibers and ipsilateral cerebral and coma (Fig. 118-7). DAI most often occurs in the setting of rapid,
peduncle compression resulting in the classic findings of an ipsilateral high magnitude acceleration or deceleration. DAI occurs in more than
dilated and fixed pupil with contralateral hemiparesis. Less commonly, 50% of all severe head trauma and in more than 85% of the subset
if the brain stem is displaced against the tentorium on the side opposite
A B
FIGURE 118-7. This patient was a pedestrian hit by a car. He suffered severe diffuse
axonal injury (DAI). DAI may present with essentially normal imaging that is disproportionate
to the severity of the clinical examination. However, this patient exhibited typical DAI findings
on CT. A. Corticomedullary junction (red arrows) and deep white matter and basal ganglia
(green arrow) hemorrhage. There is also blood within the occipital horns of the ventricle (black
arrow). B. The patient also exhibited a midbrain hemorrhage (blue arrow). Deep or midline
FIGURE 118-5. CT scan from a patient with diffuse injury and traumatic subarachnoid hemor- hemorrhages such as those in the ventricle and corpus callosum are often indicative of severe
rhage in bilateral sylvian fissures (red arrows) and inter hemispheric fissure and sulci (green arrow). brain disruption due to shearing forces.
section10.indd 1123 1/20/2015 9:20:14 AM