
Page 464 - Textbook of Pathology, 6th Edition
P. 464
448
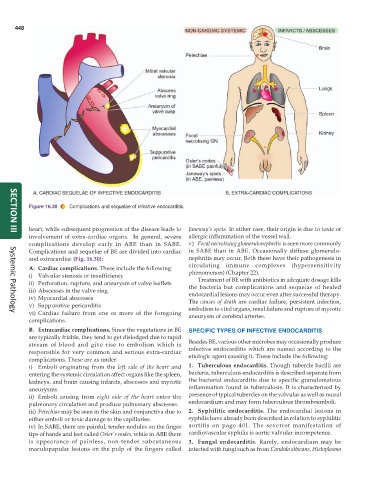
Figure 16.30 Complications and sequelae of infective endocarditis.
heart, while subsequent progression of the disease leads to Janeway’s spots. In either case, their origin is due to toxic or
SECTION III
involvement of extra-cardiac organs. In general, severe allergic inflammation of the vessel wall.
complications develop early in ABE than in SABE. v) Focal necrotising glomerulonephritis is seen more commonly
Complications and sequelae of BE are divided into cardiac in SABE than in ABE. Occasionally diffuse glomerulo-
and extracardiac (Fig. 16.30): nephritis may occur. Both these have their pathogenesis in
circulating immune complexes (hypersensitivity
A. Cardiac complications. These include the following:
i) Valvular stenosis or insufficiency phenomenon) (Chapter 22).
ii) Perforation, rupture, and aneurysm of valve leaflets Treatment of BE with antibiotics in adequate dosage kills
iii) Abscesses in the valve ring the bacteria but complications and sequelae of healed
endocardial lesions may occur even after successful therapy.
iv) Myocardial abscesses The causes of death are cardiac failure, persistent infection,
v) Suppurative pericarditis embolism to vital organs, renal failure and rupture of mycotic
vi) Cardiac failure from one or more of the foregoing aneurysm of cerebral arteries.
Systemic Pathology
complications.
B. Extracardiac complications. Since the vegetations in BE SPECIFIC TYPES OF INFECTIVE ENDOCARDITIS
are typically friable, they tend to get dislodged due to rapid
stream of blood and give rise to embolism which is Besides BE, various other microbes may occasionally produce
responsible for very common and serious extra-cardiac infective endocarditis which are named according to the
complications. These are as under: etiologic agent causing it. These include the following:
i) Emboli originating from the left side of the heart and 1. Tuberculous endocarditis. Though tubercle bacilli are
entering the systemic circulation affect organs like the spleen, bacteria, tuberculous endocarditis is described separate from
kidneys, and brain causing infarcts, abscesses and mycotic the bacterial endocarditis due to specific granulomatous
aneurysms. inflammation found in tuberculosis. It is characterised by
ii) Emboli arising from right side of the heart enter the presence of typical tubercles on the valvular as well as mural
pulmonary circulation and produce pulmonary abscesses. endocardium and may form tuberculous thromboemboli.
iii) Petechiae may be seen in the skin and conjunctiva due to 2. Syphilitic endocarditis. The endocardial lesions in
either emboli or toxic damage to the capillaries. syphilis have already been described in relation to syphilitic
iv) In SABE, there are painful, tender nodules on the finger aortitis on page 401. The severest manifestation of
tips of hands and feet called Osler’s nodes, while in ABE there cardiovascular syphilis is aortic valvular incompetence.
is appearance of painless, non-tender subcutaneous 3. Fungal endocarditis. Rarely, endocardium may be
maculopapular lesions on the pulp of the fingers called infected with fungi such as from Candida albicans, Histoplasma