
Page 852 - Textbook of Pathology, 6th Edition
P. 852
836 bone rarefaction to prominent areas of bone destruction PATHOGENESIS. Renal osteodystrophy involves two
with cyst formation or brown tumours. main events: hyperphosphataemia and hypocalcaemia which,
Grossly, there are focal areas of erosion of cortical bone in turn, leads to parathormone elaboration and resultant
and loss of lamina dura at the roots of teeth. osteoclastic activity and major lesions of renal osteo-
Histologically, the following sequential changes appear dystrophy—osteomalacia (rickets in children), secondary
over a period of time: hyperparathyroidism, osteitis fibrosa cystica, osteosclerosis
Earliest change is demineralisation and increased bone and metastatic calcification.
resorption beginning at the subperiosteal and endosteal The mechanisms underlying renal osteodystrophy are
surface of the cortex and then spreading to the trabecular schematically illustrated in Fig. 28.6 and briefly outlined
bone. below:
There is replacement of bone and bone marrow by 1. Hyperphosphataemia: In CRF, there is impaired renal
fibrosis coupled with increased number of bizarre excretion of phosphate, causing phosphate retention and
osteoclasts at the surfaces of moth-eaten trabeculae and hyperphosphataemia. Hyperphosphataemia, in turn, causes
cortex (osteitis fibrosa). hypocalcaemia which is responsible for secondary
As a result of increased resorption, microfractures and hyperparathyroidism.
microhaemorrhages occur in the marrow cavity leading 2. Hypocalcaemia: Hypocalcaemia may also result from the
to development of cysts (osteitis fibrosa cystica). following:
Haemosiderin-laden macrophages and multinucleate Due to renal dysfunction, there is decreased conversion
giant cells appear at the areas of haemorrhages producing of vitamin D metabolite 25(OH) cholecalciferol to its active
an appearance termed as ‘brown tumour’ or ‘reparative giant form 1,25 (OH) cholecalciferol.
2
cell granuloma of hyperparathyroidism’ requiring Reduced intestinal absorption of calcium.
differentiation from giant cell tumour or osteoclastoma
(page 846). However, the so-called brown tumours, unlike 3. Parathormone secretion: Hypocalcaemia stimulates
osteoclastoma, are not true tumours but instead regress secretion of parathormone, eventually leading to secondary
or disappear on surgical removal of hyperplastic or hyperparathyroidism which, in turn, causes increased
adenomatous parathyroid tissue. osteoclastic activity.
4. Metabolic acidosis: As a result of decreased renal
Renal Osteodystrophy (Metabolic Bone Disease) function, acidosis sets in which may cause osteoporosis and
Renal osteodystrophy is a loosely used term that encom- bone decalcification.
SECTION III
passes a number of skeletal abnormalities appearing in cases 5. Calcium phosphorus product > 70: When the product of
of chronic renal failure and in patients treated by dialysis for biochemical value of calcium and phosphate is higher than
several years (page 656). Renal osteodystrophy is more 70, metastatic calcification may occur at extraosseous sites.
common in children than in adults. Clinical symptoms of 6. Dialysis-related metabolic bone disease: Long-term dia-
bone disease in advanced renal failure appear in less than lysis employing use of aluminium-containing dialysate is
10% of patients but radiologic and histologic changes are currently considered to be a major cause of metabolic bone
observed in fairly large proportion of cases. lesions. Aluminium interferes with deposition of calcium
Systemic Pathology
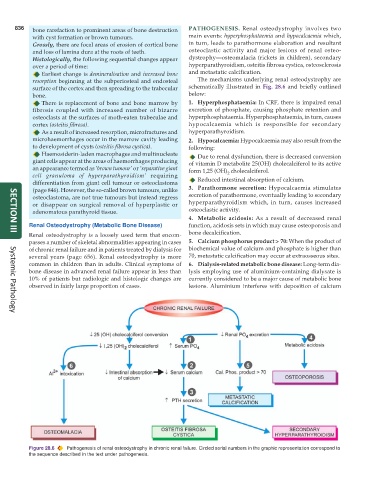
Figure 28.6 Pathogenesis of renal osteodystrophy in chronic renal failure. Circled serial numbers in the graphic representation correspond to
the sequence described in the text under pathogenesis.