
Page 436 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 436
306 PART 3: Cardiovascular Disorders
Echocardiography is extremely useful in the differential diagnosis, Myocardial dysfunction
which includes free wall rupture, ventricular septal rupture, and infarct
extension with pump failure. Hemodynamic monitoring with pulmo- Systolic Diastolic
nary artery catheterization may also be helpful. Management includes
afterload reduction with nitroprusside and intra-aortic balloon pumping ↑ LVEDP
as temporizing measures. Inotropic or vasopressor therapy may also be ↓ Cardiac output Pulmonary congestion
needed to support cardiac output and blood pressure. Definitive therapy, ↓ Stroke volume
however, is surgical valve repair or replacement, which should be under-
taken as soon as possible since clinical deterioration can be sudden. 130-132 ↓ Systemic Hypotension
■ RIGHT VENTRICULAR INFARCTION perfusion ↓ Coronary Hypoxemia
Right ventricular infarction occurs in up to 30% of patients with infe- perfusion
rior infarction and is clinically significant in 10%. The combination pressure
133
of a clear chest x-ray with jugular venous distention in a patient with Compensatory
an inferior wall MI should lead to the suspicion of a coexisting right vasoconstriction; Ischemia
ventricular infarct. The diagnosis is substantiated by demonstration Fluid retention Progressive
of ST segment elevation in the right precordial leads (V to V ) or myocardial
5R
3R
by characteristic hemodynamic findings on right heart catheterization dysfunction
(elevated right atrial and right ventricular end-diastolic pressures with
normal to low pulmonary artery occlusion pressure and low cardiac Death
output). Echocardiography can demonstrate depressed right ventricu-
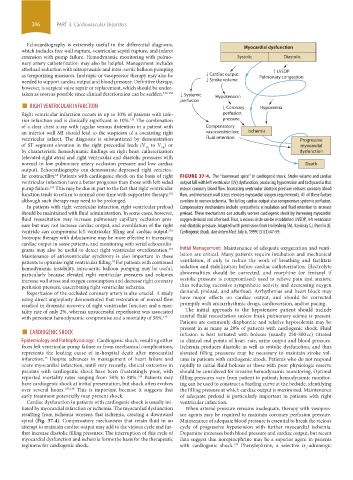
lar contractility. Patients with cardiogenic shock on the basis of right FIGURE 37-4. The “downward spiral” in cardiogenic shock. Stroke volume and cardiac
18
ventricular infarction have a better prognosis than those with left-sided output fall with left ventricular (LV) dysfunction, producing hypotension and tachycardia that
pump failure. This may be due in part to the fact that right ventricular reduce coronary blood flow. Increasing ventricular diastolic pressure reduces coronary blood
133
function tends to return to normal over time with supportive therapy, flow, and increased wall stress elevates myocardial oxygen requirements. All of these factors
134
although such therapy may need to be prolonged. combine to worsen ischemia. The falling cardiac output also compromises systemic perfusion.
In patients with right ventricular infarction, right ventricular preload Compensatory mechanisms include sympathetic stimulation and fluid retention to increase
should be maintained with fluid administration. In some cases, however, preload. These mechanisms can actually worsen cardiogenic shock by increasing myocardial
fluid resuscitation may increase pulmonary capillary occlusion pres- oxygen demand and afterload. Thus, a vicious circle can be established. LVEDP, left ventricular
sure but may not increase cardiac output, and overdilation of the right end-diastolic pressure. Adapted with permission from Hollenberg SM, Kavinsky CJ, Parrillo JE.
ventricle can compromise left ventricular filling and cardiac output. Cardiogenic shock. Ann Intern Med. July 6, 1999;131(1):47-59.
134
Inotropic therapy with dobutamine may be more effective in increasing
cardiac output in some patients, and monitoring with serial echocardio-
grams may also be useful to detect right ventricular overdistention. Initial Management: Maintenance of adequate oxygenation and venti-
134
Maintenance of atrioventricular synchrony is also important in these lation are critical. Many patients require intubation and mechanical
patients to optimize right ventricular filling. For patients with continued ventilation, if only to reduce the work of breathing and facilitate
18
hemodynamic instability, intra-aortic balloon pumping may be useful, sedation and stabilization before cardiac catheterization. Electrolyte
particularly because elevated right ventricular pressures and volumes abnormalities should be corrected, and morphine (or fentanyl if
increase wall stress and oxygen consumption and decrease right coronary systolic pressure is compromised) used to relieve pain and anxiety,
perfusion pressure, exacerbating right ventricular ischemia. thus reducing excessive sympathetic activity and decreasing oxygen
Reperfusion of the occluded coronary artery is also crucial. A study demand, preload, and afterload. Arrhythmias and heart block may
using direct angioplasty demonstrated that restoration of normal flow have major effects on cardiac output, and should be corrected
resulted in dramatic recovery of right ventricular function and a mor- promptly with antiarrhythmic drugs, cardioversion, and/or pacing.
tality rate of only 2%, whereas unsuccessful reperfusion was associated The initial approach to the hypotensive patient should include
with persistent hemodynamic compromise and a mortality of 58%. 135 careful fluid resuscitation unless frank pulmonary edema is present.
Patients are commonly diaphoretic and relative hypovolemia may be
■ CARDIOGENIC SHOCK present in as many as 20% of patients with cardiogenic shock. Fluid
infusion is best initiated with boluses (usually 250-500 cc) titrated
Epidemiology and Pathophysiology: Cardiogenic shock, resulting either to clinical end points of heart rate, urine output and blood pressure.
from left ventricular pump failure or from mechanical complications, Ischemia produces diastolic as well as systolic dysfunction, and thus
represents the leading cause of in-hospital death after myocardial elevated filling pressures may be necessary to maintain stroke vol-
infarction. Despite advances in management of heart failure and ume in patients with cardiogenic shock. Patients who do not respond
13
acute myocardial infarction, until very recently, clinical outcomes in rapidly to initial fluid boluses or those with poor physiologic reserve
patients with cardiogenic shock have been frustratingly poor, with should be considered for invasive hemodynamic monitoring. Optimal
136
reported mortality rates ranging from 50% to 80%. Patients may filling pressures vary from patient to patient; hemodynamic monitor-
have cardiogenic shock at initial presentation, but shock often evolves ing can be used to construct a Starling curve at the bedside, identifying
over several hours. 137,138 This is important because it suggests that the filling pressure at which cardiac output is maximized. Maintenance
early treatment potentially may prevent shock. of adequate preload is particularly important in patients with right
Cardiac dysfunction in patients with cardiogenic shock is usually ini- ventricular infarction.
tiated by myocardial infarction or ischemia. The myocardial dysfunction When arterial pressure remains inadequate, therapy with vasopres-
resulting from ischemia worsens that ischemia, creating a downward sor agents may be required to maintain coronary perfusion pressure.
spiral (Fig. 37-4). Compensatory mechanisms that retain fluid in an Maintenance of adequate blood pressure is essential to break the vicious
attempt to maintain cardiac output may add to the vicious cycle and fur- cycle of progressive hypotension with further myocardial ischemia.
ther increase diastolic filling pressures. The interruption of this cycle of Dopamine increases both blood pressure and cardiac output, but recent
myocardial dysfunction and ischemia forms the basis for the therapeutic data suggest that norepinephrine may be a superior agent in patients
regimens for cardiogenic shock. with cardiogenic shock. Phenylephrine, a selective α -adrenergic
139
1
section03.indd 306 1/23/2015 2:07:23 PM