
Page 441 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 441
CHAPTER 38: Acute Right Heart Syndromes 311
treated currently or within the previous 6 months) and laboratory results,
especially serum D-dimer level, can be useful in excluding pulmonary
embolism as a likely cause. The performance characteristics of clinical
20
prediction rules (Wells score or revised Geneva score) in combination
with D-dimer assays for the diagnosis of PE are discussed in Chap. 39.
21
Electrocardiography: Electrocardiographic (ECG) evidence of RV failure
in the context of pulmonary hypertension includes sinus tachycardia
or atrial fibrillation, right axis deviation or a rightward shift in axis, right
atrial enlargement, right ventricular hypertrophy, right bundle-branch
block (RBBB), right precordial T-wave inversions (leads III and aVF or in
leads V -V ), and the S Q T pattern. Additional configurations include a
3
3
4
1
1
Qr pattern in lead V , S waves in lead I and aVL >1.5 mm and Q waves in
1
leads III and aVF, but not in lead II. Reports of typical ECG changes vary
5
significantly suggesting relative insensitivity in the performance charac-
22
teristics of the 12-lead ECG in broad groups of mixed severity right heart
syndrome patients. However, in patients with hemodynamically significant
pulmonary embolism, the likelihood of suggestive electrocardiographic
findings is probably much higher. For example, among 49 patients with PE
(all of whom had RV dilation and tricuspid regurgitation by echocardiogra-
phy), 37 (76%) had electrocardiographic abnormalities strongly suggestive
of PE, including at least three of the following: incomplete or complete
RBBB; S waves greater than 1.5 mm in leads I and aVL; shift of the precor-
dial transition zone to V ; Q waves in leads III and aVF, but not lead II; right
5
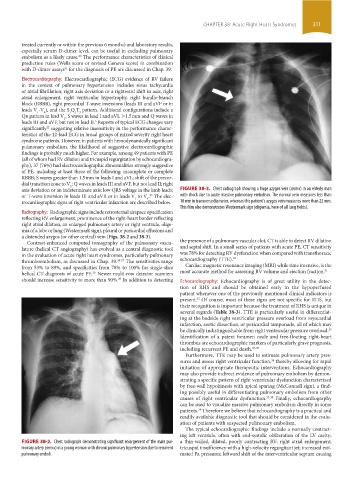
axis deviation or an indeterminate axis; low QRS voltage in the limb leads; FIGURE 38-3. Chest radiograph showing a huge azygos vein (arrow) in an elderly man
or T-wave inversion in leads III and aVR or in leads V to V . The elec- with shock due to acute massive pulmonary embolism. The normal vein measures less than
23
4
1
trocardiographic signs of right ventricular infarction are described below. 10 mm in transverse diameter, whereas this patient’s azygos vein measures more than 22 mm.
This film also demonstrates Westermark sign (oligemia, here of all lung fields).
Radiography: Radiographic signs include retrosternal airspace opacification
reflecting RV enlargement, prominence of the right-heart border reflecting
right atrial dilation, an enlarged pulmonary artery or right ventricle, olige-
mia of a lobe or lung (Westermark sign), pleural or pericardial effusions and
a distended azygos (or other central) vein (Figs. 38-2 and 38-3).
Contrast-enhanced computed tomography of the pulmonary vascu- the presence of a pulmonary vascular clot, CT is able to detect RV dilation
lature (helical CT angiography) has evolved as a central diagnostic tool and septal shift. In a small series of patients with acute PE, CT sensitivity
in the evaluation of acute right heart syndromes, particularly pulmonary was 78% for detecting RV dysfunction when compared with transthoracic
thromboembolism, as discussed in Chap. 39. 24-27 The sensitivities range echocardiography (TTE). 30
from 53% to 89%, and specificities from 78% to 100% for single-slice Cardiac magnetic resonance imaging (MRI) while time intensive, is the
helical CT diagnosis of acute PE. Newer multi-row detector scanners most accurate method for assessing RV volume and ejection fraction. 31
28
should increase sensitivity to more than 90%. In addition to detecting Echocardiography: Echocardiography is of great utility in the detec-
29
tion of RHS and should be obtained early in the hypoperfused
patient whenever one of the previously mentioned clinical indicators is
present. Of course, most of these signs are not specific for RHS, but
32
their recognition is important because the treatment of RHS is unique in
several regards (Table 38-3). TTE is particularly useful in differentiat-
ing at the bedside right ventricular pressure overload from myocardial
infarction, aortic dissection, or pericardial tamponade, all of which may
be clinically indistinguishable from right ventricular pressure overload.
33
Identification of a patent foramen ovale and free-floating right-heart
thrombus are echocardiographic markers of particularly grave prognosis,
including recurrent PE and death. 33-35
Furthermore, TTE may be used to estimate pulmonary artery pres-
sures and assess right ventricular function, thereby allowing for rapid
36
initiation of appropriate therapeutic interventions. Echocardiography
may also provide indirect evidence of pulmonary embolism by demon-
strating a specific pattern of right ventricular dysfunction characterized
by free-wall hypokinesis with apical sparing (McConnell sign), a find-
ing possibly useful in differentiating pulmonary embolism from other
causes of right ventricular dysfunction. 32-38 Finally, echocardiography
can be used to visualize massive pulmonary embolism directly in some
34
patients. Therefore we believe that echocardiography is a practical and
readily available diagnostic tool that should be considered in the evalu-
ation of patients with suspected pulmonary embolism.
The typical echocardiographic findings include a normally contract-
ing left ventricle, often with end-systolic obliteration of the LV cavity;
FIGURE 38-2. Chest radiograph demonstrating significant enlargement of the main pul- a thin-walled, dilated, poorly contracting RV; right atrial enlargement;
monary artery (arrow) in a young woman with chronic pulmonary hypertension due to recurrent tricuspid insufficiency with a high-velocity regurgitant jet; increased esti-
pulmonary emboli. mated Pa pressures; leftward shift of the interventricular septum causing
section03.indd 311 1/23/2015 2:07:26 PM