
Page 190 - Clinical Anatomy
P. 190
ECA3 7/18/06 6:45 PM Page 175
The bones and joints of the upper limb 175
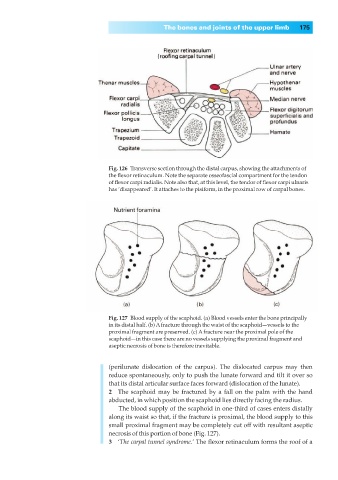
Fig. 126◊Transverse section through the distal carpus, showing the attachments of
the flexor retinaculum. Note the separate osseofascial compartment for the tendon
of flexor carpi radialis. Note also that, at this level, the tendor of flexor carpi ulnaris
has ‘disappeared’. It attaches to the pisiform, in the proximal row of carpal bones.
Fig. 127◊Blood supply of the scaphoid. (a) Blood vessels enter the bone principally
in its distal half. (b) Afracture through the waist of the scaphoid—vessels to the
proximal fragment are preserved. (c) Afracture near the proximal pole of the
scaphoid—in this case there are no vessels supplying the proximal fragment and
aseptic necrosis of bone is therefore inevitable.
(perilunate dislocation of the carpus). The dislocated carpus may then
reduce spontaneously, only to push the lunate forward and tilt it over so
that its distal articular surface faces forward (dislocation of the lunate).
2◊◊The scaphoid may be fractured by a fall on the palm with the hand
abducted, in which position the scaphoid lies directly facing the radius.
The blood supply of the scaphoid in one-third of cases enters distally
along its waist so that, if the fracture is proximal, the blood supply to this
small proximal fragment may be completely cut off with resultant aseptic
necrosis of this portion of bone (Fig. 127).
3◊◊‘The carpal tunnel syndrome.’ The flexor retinaculum forms the roof of a