
Page 230 - Clinical Anatomy
P. 230
ECA4 7/18/06 6:47 PM Page 215
The anatomy and surface markings of the lower limb 215
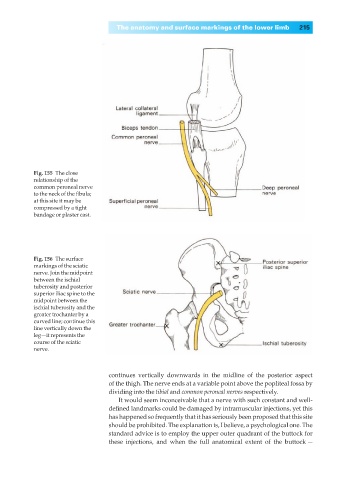
Fig. 155◊The close
relationship of the
common peroneal nerve
to the neck of the fibula;
at this site it may be
compressed by a tight
bandage or plaster cast.
Fig. 156◊The surface
markings of the sciatic
nerve. Join the midpoint
between the ischial
tuberosity and posterior
superior iliac spine to the
midpoint between the
ischial tuberosity and the
greater trochanter by a
curved line; continue this
line vertically down the
leg—it represents the
course of the sciatic
nerve.
continues vertically downwards in the midline of the posterior aspect
of the thigh. The nerve ends at a variable point above the popliteal fossa by
dividing into the tibial and common peroneal nerves respectively.
It would seem inconceivable that a nerve with such constant and well-
defined landmarks could be damaged by intramuscular injections, yet this
has happened so frequently that it has seriously been proposed that this site
should be prohibited. The explanation is, I believe, a psychological one. The
standard advice is to employ the upper outer quadrant of the buttock for
these injections, and when the full anatomical extent of the buttock —