
Page 369 - Cardiac Nursing
P. 369
LWBK340-c16_p333-387.qxd 6/30/09 12:16 AM Page 345 Aptara Inc.
C HAP TE R 1 6 / Arrhythmias and Conduction Disturbances 345
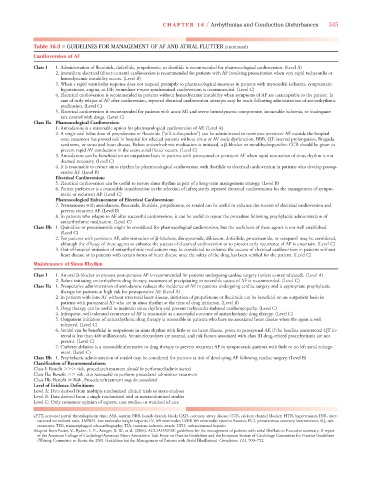
Table 16-3 ■ GUIDELINES FOR MANAGEMENT OF AF AND ATRIAL FLUTTER (continued)
Cardioversion of AF
Class I 1. Administration of flecainide, dofetilide, propafenone, or ibutilide is recommended for pharmacological cardioversion. (Level A)
2. Immediate electrical (direct-current) cardioversion is recommended for patients with AF involving preexcitation when very rapid tachycardia or
hemodynamic instability occurs. (Level B)
3. When a rapid ventricular response does not respond promptly to pharmacological measures in patients with myocardial ischemia, symptomatic
hypotension, angina, or HF, immediate r-wave synchronized cardioversion is recommended. (Level C)
4. Electrical cardioversion is recommended in patients without hemodynamic instability when symptoms of AF are unacceptable to the patient. In
case of early relapse of AF after cardioversion, repeated electrical cardioversion attempts may be made following administration of antiarrhythmic
medication. (Level C)
5. Electrical cardioversion is recommended for patients with acute MI and severe hemodynamic compromise, intractable ischemia, or inadequate
rate control with drugs. (Level C)
Class IIa Pharmacological Cardioversion:
1. Amiodarone is a reasonable option for pharmacological cardioversion of AF. (Level A)
2. A single oral bolus dose of propafenone or flecainide (“pill-it-the-pocket”) can be administered to terminate persistent AF outside the hospital
once treatment has proved safe in hospital for selected patients without sinus or AV node dysfunction, BBB, QT-interval prolongation, Brugada
syndrome, or structural heart disease. Before antiarrhythmic medication is initiated, a -blocker or nondihydropyridine CCB should be given to
prevent rapid AV conduction in the event atrial flutter occurs. (Level C)
3. Amiodarone can be beneficial on an outpatient basis in patients with paroxysmal or persistent AF when rapid restoration of sinus rhythm is not
deemed necessary. (Level C)
4. It is reasonable to restore sinus rhythm by pharmacological cardioversion with ibutilide or electrical cardioversion in patients who develop postop-
erative AF. (Level B)
Electrical Cardioversion:
5. Electrical cardioversion can be useful to restore sinus rhythm as part of a long-term management strategy. (Level B)
6. Patient preference is a reasonable consideration in the selection of infrequently repeated electrical cardioversions for the management of sympto-
matic or recurrent AF. (Level C)
Pharmacological Enhancement of Electrical Cardioversion:
7. Pretreatment with amiodarone, flecainide, ibutilide, propafenone, or sotalol can be useful to enhance the success of electrical cardioversion and
prevent recurrent AF. (Level B)
8. In patients who relapse to AF after successful cardioversion, it can be useful to repeat the procedure following prophylactic administration of
antiarrhythmic medication. (Level C)
Class IIb 1. Quinidine or procainamide might be considered for pharmacological cardioversion, but the usefulness of these agents is not well established.
(Level C)
2. For patients with persistent AF, administration of -blockers, disopyramide, diltiazem, dofetilide, procainamide, or verapamil may be considered,
although the efficacy of these agents to enhance the success of electrical cardioversion or to prevent early recurrence of AF is uncertain. (Level C)
3. Out-of-hospital initiation of antiarrhythmic medications may be considered to enhance the success of electrical cardioversion in patients without
heart disease or in patients with certain forms of heart disease once the safety of the drug has been verified for the patient. (Level C)
Maintenance of Sinus Rhythm
Class I 1. An oral -blocker to prevent postoperative AF is recommended for patients undergoing cardiac surgery (unless contraindicated). (Level A)
2. Before initiating antiarrhythmic drug therapy, treatment of precipitating or reversible causes of AF is recommended. (Level C)
Class IIa 1. Preoperative administration of amiodarone reduces the incidence of AF in patients undergoing cardiac surgery and is appropriate prophylactic
therapy for patients at high risk for postoperative AF. (Level A)
2. In patients with lone AF without structural heart disease, initiation of propafenone or flecainide can be beneficial on an outpatient basis in
patients with paroxysmal AF who are in sinus rhythm at the time of drug initiation. (Level B)
3. Drug therapy can be useful to maintain sinus rhythm and prevent tachycardia-induced cardiomyopathy. (Level C)
4. Infrequent, well-tolerated recurrence of AF is reasonable as a successful outcome of antiarrhythmic drug therapy. (Level C)
5. Outpatient initiation of antiarrhythmic drug therapy is reasonable in patients who have no associated heart disease when the agent is well
tolerated. (Level C)
6. Sotalol can be beneficial in outpatients in sinus rhythm with little or no heart disease, prone to paroxysmal AF, if the baseline uncorrected QT in-
terval is less than 460 milliseconds. Serum electrolytes are normal, and risk factors associated with class III drug-related proarrhythmia are not
present. (Level C)
7. Catheter ablation is a reasonable alternative to drug therapy to prevent recurrent AF in symptomatic patients with little or no left atrial enlarge-
ment. (Level C)
Class IIb 1. Prophylactic administration of sotalol may be considered for patients at risk of developing AF following cardiac surgery. (Level B)
Classification of Recommendations:
Class I: Benefit risk, procedure/treatment should be performed/administered
Class IIa: Benefit risk, it is reasonable to perform procedure/ administer treatment
Class IIb: Benefit Risk, Procedure/treatment may be considered
Level of Evidence Definitions:
Level A: Data derived from multiple randomized clinical trials or meta-analyses
Level B: Data derived from a single randomized trial or nonrandomized studies
Level C: Only consensus opinion of experts, case studies, or standard of care
aPTT, activated partial thromboplastin time; ASA, aspirin; BBB, bundle-branch block; CAD, coronary artery disease; CCB, calcium channel blocker; HTN, hypertension; INR, inter-
national normalized ratio; LMWH, low molecular weight heparin; LV, left ventricular; LVEF, left ventricular ejection fraction; PCI, percutaneous coronary interventions; SQ, sub-
cutaneous; TEE, transesophageal echocardiography; TIA, transient ischemic attack; UFH: unfractionated heparin.
Adapted from Fuster, V., Ryden, L. E., Asinger, R. W., et al. (2006). ACC/AHA/ESC guidelines for the management of patients with atrial fibrillation: Executive summary: A report
of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines
(Writing Committee to Revise the 2001 Guidelines for the Management of Patients with Atrial Fibrillation). Circulation, 114, 700–752.4 4