
Page 717 - Cardiac Nursing
P. 717
tar
49
09
693
AM
Ap
04.
5-7
p65
/1/
7
qxd
K34
0-c
28_
LWB K34 0-c 28_ p65 5-7 04. qxd 7 /1/ 09 9: 49 AM P a a g e e 693 Ap tar a a
LWB
LWBK340-c28_p655-704.qxd 7/1/09 9:9:49 AM Page 693 Aptara
P
g
C HAPTER 2 8 / Pacemakers and Implantable Defibrillators 693
Trigger
F
VF
V VF * * * * * * * * * * * * * * * * * * * * * ** * ** * ** * ** * ** * ** * ** * ** * ** * ** * ** * * ** ** * ** * ** * ** *
VS
VS VS F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F
S
VS
V VS
VS
V VS
* * * * * * * * * * – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – – –
236
236
236
236
236
236
66
2 266
2 266
248
66
66
236
238
238
248
238
2 238
238
238
238
248
238
238
238
2
238
238
238
234
234
238
238
234
234
234
238
238
234
248
266
248
266
266
248
266
26
266
234
266
26
266
2 238
2 242
242
238
2 242
242
238
238
238
2 234
238
238
234
238
62
62
62
238
238
238
2 262
4
4
4
262
262
2 262
238
238
238
38
238
23
238
38
38
38
2 238
3
3
248
238
238
238
238
238
234
23
2 234
3
23
238
238
238
490
490
28
28
280
490
2 238
2 238
238
280
280
1
280
248
248
248
248
248
248
490
490
28
248
490
490
2 238
2 262
5 512 2 2 2 490 248 280 0 0 0 238 8 8 8 2 262 238 26 6 6 6 266 236 238 2 238 23 8 8 8 8 238 2 242 2 2 2 2 262 238 2 234 4 4 4 248 234
5 512
262
2 262
262
62
512
5 512
512
62
62
1
1
3
3
3
16s 17s 18s 19s 20s 21s 22s 23s 24s
VVI VVI
us
n
n
Return to Sinus
R R Retur
R R Retur
us
us
n
Si
Si
Sinus
etu
n
n t
etu
Si
Sinus
nt
etu
* * * * * * * * * * * * * * * * * * ( (HV) ) ) ) R R Retur r r r n n nt t t t o o o o o o Sinus
(HV)
( (HV)
( (HV)
HV
HV
HV
F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F F * * * * * * VS VS V S VS VS VSS VSVS VS
VS
S
S
VS
VSS
VS
S
V VS
V VS
V VS
V VS
VSS
V VS
VSVS
VS
VS
VS
VS
VSVS
VS
VS
VS
VS
VS
VS
VS
VS
VS
V
VS
VSSVS
V VS
V VS
VS
VS
VS
VS
V
S
VS
S
S
V V VS
V
V V VS
V V VS
S
S
VS
VS
S
V VS
V VS
VS
V VS
V VS
S
– – – – – – – – – – – – – – – – – – – – – – – 7 757 V V V
7 757
757 VVV
57
57 V
2 238
453
45
453
45
5
445
5
2 238 8 2 234 238 248 8 2344 4 2 2 234 2 234 4 453 3 4 435 535 5 5 7300 0 5 500 0 4 461 457 4533 3 445
4 445
2388
4 445
445
535
53
535
2 234
3
3
2 234
730
3
3
730
53
73
73
35
34
34
2 2 234
2 234
234
234
234
5
4 435
43535
5
234
4533
4 453
46161
34
61
4 461
238
238
34
238
457
457
3
457
234
2 234
457
3
238
5 500
0
2488
24
24
5000
248
0
24s 25s 26s 27s 28s 29s 30s 31s 32s
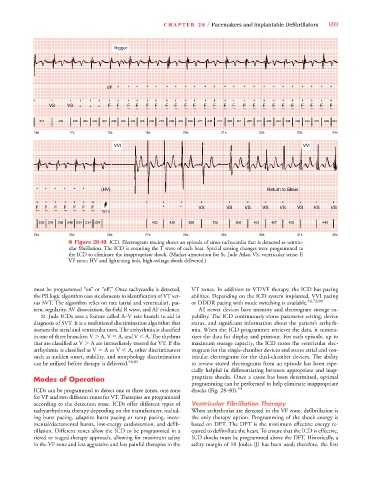
■ Figure 28-40 ICD. Electrogram tracing shows an episode of sinus tachycardia that is detected as ventric-
ular fibrillation. The ICD is counting the T wave of each beat. Special sensing changes were programmed to
the ICD to eliminate the inappropriate shock. (Marker annotation for St. Jude Atlas; VS, ventricular sense; F,
VF zone; HV and lightening bolt, high-voltage shock delivered.)
must be programmed “on” or “off.” Once tachycardia is detected, VT zones. In addition to VT/VF therapy, the ICD has pacing
the PR logic algorithm uses six elements in identification of VT ver- abilities. Depending on the ICD system implanted, VVI pacing
sus SVT. The algorithm relies on rate (atrial and ventricular), pat- or DDDR pacing with mode switching is available. 54,72,80
tern, regularity, AV dissociation, far-field R wave, and AF evidence. All newer devices have memory and electrogram storage ca-
St. Jude ICDs uses a feature called A–V rate branch to aid in pability. The ICD continuously stores parameter setting, device
diagnosis of SVT. It is a multitiered discrimination algorithm that status, and significant information about the patient’s arrhyth-
assesses the atrial and ventricular rates. The arrhythmia is classified mia. When the ICD programmer retrieves the data, it summa-
in one of three branches: V A, V A, and V A. The rhythms rizes the data for display and printout. For each episode, up to
that are classified as V A are immediately treated for VT. If the maximum storage capacity, the ICD stores the ventricular elec-
arrhythmia is classified as V A or V A, other discriminators trogram for the single-chamber devices and stores atrial and ven-
such as sudden onset, stability, and morphology discrimination tricular electrograms for the dual-chamber devices. The ability
can be utilized before therapy is delivered. 54,82 to review stored electrograms from an episode has been espe-
cially helpful in differentiating between appropriate and inap-
Modes of Operation propriate shocks. Once a cause has been determined, optimal
programming can be performed to help eliminate inappropriate
ICDs can be programmed to detect one to three zones, one zone shocks (Fig. 28-40). 54
for VF and two different zones for VT. Therapies are programmed
according to the detection zone. ICDs offer different types of Ventricular Fibrillation Therapy
tachyarrhythmia therapy depending on the manufacturer, includ- When arrhythmias are detected in the VF zone, defibrillation is
ing burst pacing, adaptive burst pacing or ramp pacing, incre- the only therapy option. Programming of the shock energy is
mental/decremental bursts, low-energy cardioversion, and defib- based on DFT. The DFT is the minimum effective energy re-
rillation. Different zones allow the ICD to be programmed in a quired to defibrillate the heart. To ensure that the ICD is effective,
tiered or staged-therapy approach, allowing for maximum safety ICD shocks must be programmed above the DFT. Historically, a
in the VF zone and less aggressive and less painful therapies in the safety margin of 10 Joules (J) has been used; therefore, the first