
Page 221 - ACCCN's Critical Care Nursing
P. 221
198 P R I N C I P L E S A N D P R A C T I C E O F C R I T I C A L C A R E
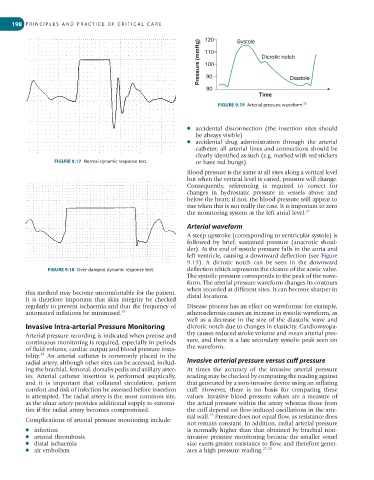
120 Systole
Pressure (mmHg) 110 Dicrotic notch
100
90
80 Diastole
Time
58
FIGURE 9.19 Arterial pressure waveform.
● accidental disconnection (the insertion sites should
be always visible)
● accidental drug administration through the arterial
catheter; all arterial lines and connections should be
clearly identified as such (e.g. marked with red stickers
FIGURE 9.17 Normal dynamic response test. or have red bungs).
Blood pressure is the same at all sites along a vertical level
but when the vertical level is varied, pressure will change.
Consequently, referencing is required to correct for
changes in hydrostatic pressure in vessels above and
below the heart; if not, the blood pressure will appear to
rise when this is not really the case. It is important to zero
the monitoring system at the left atrial level. 27
Arterial waveform
A steep upstroke (corresponding to ventricular systole) is
followed by brief, sustained pressure (anacrotic shoul-
der). At the end of systole pressure falls in the aorta and
left ventricle, causing a downward deflection (see Figure
9.19). A dicrotic notch can be seen in the downward
FIGURE 9.18 Over-damped dynamic response test. deflection which represents the closure of the aortic valve.
The systolic pressure corresponds to the peak of the wave-
form. The arterial pressure waveform changes its contours
when recorded at different sites. It can become sharper in
this method may become uncomfortable for the patient. distal locations.
It is therefore important that skin integrity be checked
regularly to prevent ischaemia and that the frequency of Disease process has an effect on waveforms: for example,
automated inflations be minimised. 33 atherosclerosis causes an increase in systolic waveform, as
well as a decrease in the size of the diastolic wave and
Invasive Intra-arterial Pressure Monitoring dicrotic notch due to changes in elasticity. Cardiomyopa-
Arterial pressure recording is indicated when precise and thy causes reduced stroke volume and mean arterial pres-
continuous monitoring is required, especially in periods sure, and there is a late secondary systolic peak seen on
of fluid volume, cardiac output and blood pressure insta- the waveform.
34
bility. An arterial catheter is commonly placed in the
radial artery, although other sites can be accessed, includ- Invasive arterial pressure versus cuff pressure
ing the brachial, femoral, dorsalis pedis and axillary arter- At times the accuracy of the invasive arterial pressure
ies. Arterial catheter insertion is performed aseptically, reading may be checked by comparing the reading against
and it is important that collateral circulation, patient that generated by a non-invasive device using an inflating
comfort and risk of infection be assessed before insertion cuff. However, there is no basis for comparing these
is attempted. The radial artery is the most common site, values. Invasive blood pressure values are a measure of
as the ulnar artery provides additional supply to extremi- the actual pressure within the artery whereas those from
ties if the radial artery becomes compromised. the cuff depend on flow-induced oscillations in the arte-
35
rial wall. Pressure does not equal flow, as resistance does
Complications of arterial pressure monitoring include:
not remain constant. In addition, radial arterial pressure
● infection is normally higher than that obtained by brachial non-
● arterial thrombosis invasive pressure monitoring because the smaller vessel
● distal ischaemia size exerts greater resistance to flow, and therefore gener-
● air embolism ates a high pressure reading. 27,35