
Page 220 - ACCCN's Critical Care Nursing
P. 220
Cardiovascular Assessment and Monitoring 197
Bedside monitor
Normal saline and
pressure bag
Macrodrip
chamber
Electrical
cable
High-
pressure Fluid-
tubing filled
tubing
for flush
Invasive
45° catheter
Roller
clamp
30°
Electrical
connection
3-way
stopcock
Disposable (air reference)
transducer
Phlebostatic
axis Manual
flush
0°
Patient with invasive catheter
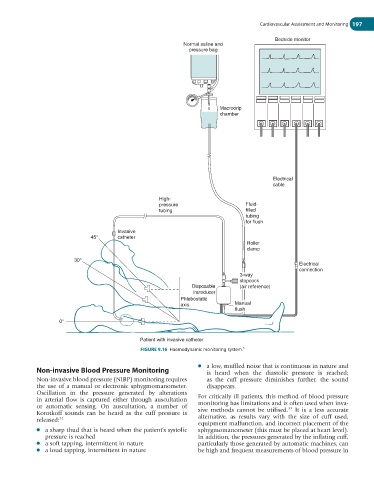
FIGURE 9.16 Haemodynamic monitoring system. 5
● a low, muffled noise that is continuous in nature and
Non-invasive Blood Pressure Monitoring is heard when the diastolic pressure is reached;
Non-invasive blood pressure (NIBP) monitoring requires as the cuff pressure diminishes further, the sound
the use of a manual or electronic sphygmomanometer. disappears.
Oscillation in the pressure generated by alterations
in arterial flow is captured either through auscultation For critically ill patients, this method of blood pressure
or automatic sensing. On auscultation, a number of monitoring has limitations and is often used when inva-
33
Korotkoff sounds can be heard as the cuff pressure is sive methods cannot be utilised. It is a less accurate
released: 32 alternative, as results vary with the size of cuff used,
equipment malfunction, and incorrect placement of the
● a sharp thud that is heard when the patient’s systolic sphygmomanometer (this must be placed at heart level).
pressure is reached In addition, the pressures generated by the inflating cuff,
● a soft tapping, intermittent in nature particularly those generated by automatic machines, can
● a loud tapping, intermittent in nature be high and frequent measurements of blood pressure in