
Page 242 - ACCCN's Critical Care Nursing
P. 242
Cardiovascular Alterations and Management 219
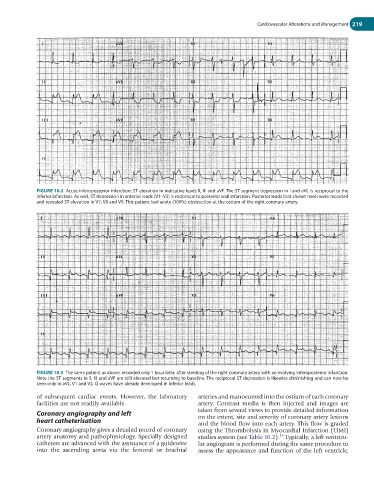
FIGURE 10.2 Acute inferoposterior infarction: ST elevation in indicative leads II, III and aVF. The ST segment depression in I and aVL is reciprocal to the
inferior infarction. As well, ST depression in anterior leads (V1–V3) is reciprocal to posterior wall infarction. Posterior leads (not shown here) were recorded
and revealed ST elevation in V7, V8 and V9. This patient had acute (100%) obstruction at the ostium of the right coronary artery.
FIGURE 10.3 The same patient as above, recorded only 1 hour later, after stenting of the right coronary artery with an evolving inferoposterior infarction.
Note the ST segments in II, III and aVF are still elevated but returning to baseline. The reciprocal ST depression is likewise diminishing and can now be
seen only in aVL, V1 and V2. Q waves have already developed in inferior leads.
of subsequent cardiac events. However, the laboratory arteries and manoeuvred into the ostium of each coronary
facilities are not readily available. artery. Contrast media is then injected and images are
Coronary angiography and left taken from several views to provide detailed information
on the extent, site and severity of coronary artery lesions
heart catheterisation and the blood flow into each artery. This flow is graded
Coronary angiography gives a detailed record of coronary using the Thrombolysis in Myocardial Infarction (TIMI)
artery anatomy and pathophysiology. Specially designed studies system (see Table 10.2). Typically, a left ventricu-
15
catheters are advanced with the assistance of a guidewire lar angiogram is performed during the same procedure to
into the ascending aorta via the femoral or brachial assess the appearance and function of the left ventricle,