
Page 482 - ACCCN's Critical Care Nursing
P. 482
Neurological Alterations and Management 459
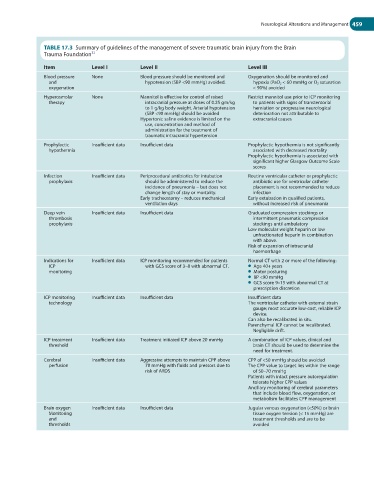
TABLE 17.3 Summary of guidelines of the management of severe traumatic brain injury from the Brain
Trauma Foundation 32
Item Level I Level II Level III
Blood pressure None Blood pressure should be monitored and Oxygenation should be monitored and
and hypotension (SBP <90 mmHg) avoided. hypoxia (PaO 2 < 60 mmHg or O 2 saturation
oxygenation < 90%) avoided
Hyperosmolar None Mannitol is effective for control of raised Restrict mannitol use prior to ICP monitoring
therapy intracranial pressure at doses of 0.25 gm/kg to patients with signs of transtentorial
to 1 g/kg body weight. Arterial hypotension herniation or progressive neurological
(SBP <90 mmHg) should be avoided deterioration not attributable to
Hypertonic saline evidence is limited on the extracranial causes
use, concentration and method of
administration for the treatment of
traumatic intracranial hypertension
Prophylactic Insufficient data Insufficient data Prophylactic hypothermia is not significantly
hypothermia associated with decreased mortality
Prophylactic hypothermia is associated with
significant higher Glasgow Outcome Scale
scores
Infection Insufficient data Periprocedural antibiotics for intubation Routine ventricular catheter or prophylactic
prophylaxis should be administered to reduce the antibiotic use for ventricular catheter
incidence of pneumonia – but does not placement is not recommended to reduce
change length of stay or mortality. infection
Early tracheostomy – reduces mechanical Early extubation in qualified patients,
ventilation days without increased risk of pneumonia
Deep vein Insufficient data Insufficient data Graduated compression stockings or
thrombosis intermittent pneumatic compression
prophylaxis stockings until ambulatory
Low molecular weight heparin or low
unfractionated heparin in combination
with above.
Risk of expansion of intracranial
haemorrhage
Indications for Insufficient data ICP monitoring recommended for patients Normal CT with 2 or more of the following:
ICP with GCS score of 3–8 with abnormal CT. ● Age 40+ years
monitoring ● Motor posturing
● BP <90 mmHg
● GCS score 9–15 with abnormal CT at
prescription discretion
ICP monitoring Insufficient data Insufficient data Insufficient data
technology The ventricular catheter with external strain
gauge; most accurate low-cost, reliable ICP
device.
Can also be recalibrated in situ.
Parenchymal ICP cannot be recalibrated.
Negligible drift.
ICP treatment Insufficient data Treatment initiated ICP above 20 mmHg A combination of ICP values, clinical and
threshold brain CT should be used to determine the
need for treatment.
Cerebral Insufficient data Aggressive attempts to maintain CPP above CPP of <50 mmHg should be avoided
perfusion 70 mmHg with fluids and pressors due to The CPP value to target lies within the range
risk of ARDS of 50–70 mmHg
Patients with intact pressure autoregulation
tolerate higher CPP values
Ancillary monitoring of cerebral parameters
that include blood flow, oxygenation, or
metabolism facilitates CPP management
Brain oxygen Insufficient data Insufficient data Jugular venous oxygenation (<50%) or brain
Monitoring tissue oxygen tension (< 15 mmHg) are
and treatment thresholds and are to be
thresholds avoided