
Page 417 - Concise Pathology for Exam Preparation ( PDFDrive )
P. 417
402
402 SECTION II Diseases of Organ Systems
• Racial factors
More common in Blacks, Americans and Indians
• Geographical influence
More prevalent in Japan, Finland and Iceland
Location
• Pylorus and antrum (50–60%)
• Cardia (25%)
• Body and fundus (15–25%)
Less curvature is involved more often as compared to greater curvature and most com-
mon location is lesser curvature of antropyloric region.
Classification
1. Microscopic or histological (Lauren) classification
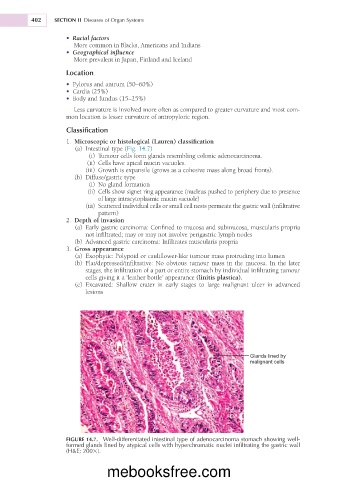
(a) Intestinal type (Fig. 14.7)
(i) Tumour cells form glands resembling colonic adenocarcinoma.
(ii) Cells have apical mucin vacuoles.
(iii) Growth is expansile (grows as a cohesive mass along broad fronts).
(b) Diffuse/gastric type
(i) No gland formation
(ii) Cells show signet ring appearance (nucleus pushed to periphery due to presence
of large intracytoplasmic mucin vacuole)
(iii) Scattered individual cells or small cell nests permeate the gastric wall (infiltrative
pattern)
2. Depth of invasion
(a) Early gastric carcinoma: Confined to mucosa and submucosa, muscularis propria
not infiltrated; may or may not involve perigastric lymph nodes
(b) Advanced gastric carcinoma: Infiltrates muscularis propria
3. Gross appearance
(a) Exophytic: Polypoid or cauliflower-like tumour mass protruding into lumen
(b) Flat/depressed/infiltrative: No obvious tumour mass in the mucosa. In the later
stages, the infiltration of a part or entire stomach by individual infiltrating tumour
cells giving it a ‘leather bottle’ appearance (linitis plastica).
(c) Excavated: Shallow crater in early stages to large malignant ulcer in advanced
lesions
Glands lined by
malignant cells
FIGURE 14.7. Well-differentiated intestinal type of adenocarcinoma stomach showing well-
formed glands lined by atypical cells with hyperchromatic nuclei infiltrating the gastric wall
(H&E; 2003).
mebooksfree.com