
Page 485 - Concise Pathology for Exam Preparation ( PDFDrive )
P. 485
470 SECTION II Diseases of Organ Systems
Thickened basement
membrane
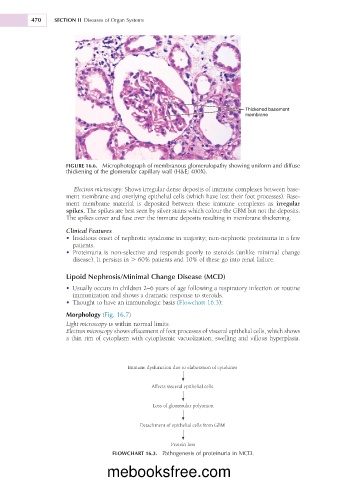
FIGURE 16.6. Microphotograph of membranous glomerulopathy showing uniform and diffuse
thickening of the glomerular capillary wall (H&E; 400X).
Electron microscopy: Shows irregular dense deposits of immune complexes between base-
ment membrane and overlying epithelial cells (which have lost their foot processes). Base-
ment membrane material is deposited between these immune complexes as irregular
spikes. The spikes are best seen by silver stains which colour the GBM but not the deposits.
The spikes cover and fuse over the immune deposits resulting in membrane thickening.
Clinical Features
• Insidious onset of nephrotic syndrome in majority; non-nephrotic proteinuria in a few
patients.
• Proteinuria is non-selective and responds poorly to steroids (unlike minimal change
disease). It persists in . 60% patients and 10% of these go into renal failure.
Lipoid Nephrosis/Minimal Change Disease (MCD)
• Usually occurs in children 2–6 years of age following a respiratory infection or routine
immunization and shows a dramatic response to steroids.
• Thought to have an immunologic basis (Flowchart 16.3):
Morphology (Fig. 16.7)
Light microscopy is within normal limits.
Electron microscopy shows effacement of foot processes of visceral epithelial cells, which shows
a thin rim of cytoplasm with cytoplasmic vacuolization, swelling and villous hyperplasia.
Immune dysfunction due to elaboration of cytokines
Affects visceral epithelial cells
Loss of glomerular polyanion
Detachment of epithelial cells from GBM
Protein loss
FLOWCHART 16.3. Pathogenesis of proteinuria in MCD.
mebooksfree.com