
Page 2608 - Hematology_ Basic Principles and Practice ( PDFDrive )
P. 2608
Chapter 160 The Spleen and Its Disorders 2321
and examination under interference optics should reveal endocytic 1.0
vesicles containing hemoglobin, ferritin, and remnants of mitochon- HbSS
dria. These form in mature erythrocytes and are normally removed by 0.9
the functioning spleen. The number of pitted cells (not the number
of pits per cell) is inversely proportional to splenic function, with
14
normal persons having less than 2% pitted cells. The absence of 0.8 HbS/b thal
0
Howell-Jolly bodies on a peripheral blood smear cannot be used as
evidence of adequate splenic immune function. 15 0.7
ASPLENIA AND HYPOSPLENIA 0.6
Congenital asplenia may be an isolated lesion or associated with Percentage of Patients with “pocked” RBC >3.5% 0.5
severe cyanotic congenital heart disease and bilateral right-sidedness. HbSC
Life-threatening cardiac lesions, including transposition of the great 0.4
vessels, pulmonary artery atresia or stenosis, septal defects, anomalous
venous drainage, and a single atrioventricular valve, are components 0.3
of bilateral right-sidedness. The liver is central, and both lungs have
+
three lobes. The peripheral blood smear shows Howell-Jolly bodies HbS/b thal
and other signs of hyposplenism. There is considerable variation in 0.2
the anatomic and functional findings, and it is difficult to predict
with accuracy the degree of splenic dysfunction on the basis of the 0.1
anatomy alone. Children who survive the cardiac difficulties in the
neonatal period have a significant incidence of sepsis secondary to a 0.0
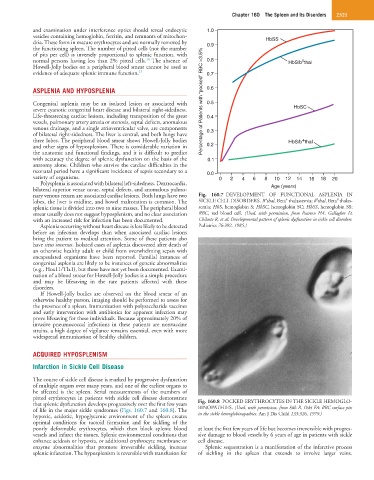
variety of organisms. 0 2 4 6 8 10 12 14 16 18 20
Polysplenia is associated with bilateral left-sidedness. Dextrocardia,
bilateral superior venae cavae, septal defects, and anomalous pulmo- Age (years)
nary venous return are associated cardiac lesions. Both lungs have two Fig. 160.7 DEVELOPMENT OF FUNCTIONAL ASPLENIA IN
+
+
0
0
lobes, the liver is midline, and bowel malrotation is common. The SICKLE CELL DISORDERS. B thal, Beta thalassemia; b thal, Beta thalas-
splenic tissue is divided into two to nine masses. The peripheral blood semia; HbS, hemoglobin S; HbSC, hemoglobin SC; HbSS, hemoglobin SS;
smear usually does not suggest hyposplenism, and no clear association RBC, red blood cell. (Used, with permission, from Pearson HA, Gallagher D,
with an increased risk for infection has been documented. Chilcote R, et al: Developmental pattern of splenic dysfunction in sickle cell disorders.
Asplenia occurring without heart disease is less likely to be detected Pediatrics 76:392, 1985.)
before an infection develops than when associated cardiac lesions
bring the patient to medical attention. Some of these patients also
have situs inversus. Isolated cases of asplenia discovered after death of
an otherwise healthy adult or child from overwhelming sepsis with
encapsulated organisms have been reported. Familial instances of
congenital asplenia are likely to be instances of genetic abnormalities
(e.g., Hox11/Tlx1), but these have not yet been documented. Exami-
nation of a blood smear for Howell-Jolly bodies is a simple procedure
and may be lifesaving in the rare patients affected with these
disorders.
If Howell-Jolly bodies are observed on the blood smear of an
otherwise healthy person, imaging should be performed to assess for
the presence of a spleen. Immunization with polysaccharide vaccines
and early intervention with antibiotics for apparent infection may
prove lifesaving for these individuals. Because approximately 20% of
invasive pneumococcal infections in these patients are nonvaccine
strains, a high degree of vigilance remains essential, even with more
widespread immunization of healthy children.
ACQUIRED HYPOSPLENISM
Infarction in Sickle Cell Disease
The course of sickle cell disease is marked by progressive dysfunction
of multiple organs over many years, and one of the earliest organs to
be affected is the spleen. Serial measurements of the numbers of
pitted erythrocytes in patients with sickle cell disease demonstrate
that splenic dysfunction develops progressively over the first few years Fig. 160.8 POCKED ERYTHROCYTES IN THE SICKLE HEMOGLO-
of life in the major sickle syndromes (Figs. 160.7 and 160.8). The BINOPATHIES. (Used, with permission, from Sills R, Oski FA: RBC surface pits
hypoxic, acidotic, hypoglycemic environment of the spleen creates in the sickle hemoglobinopathies. Am J Dis Child 133:526, 1979.)
optimal conditions for tactoid formation and for sickling of the
poorly deformable erythrocytes, which then block splenic blood at least the first few years of life but becomes irreversible with progres-
vessels and infarct the tissues. Splenic environmental conditions that sive damage to blood vessels by 6 years of age in patients with sickle
enhance acidosis or hypoxia, or additional erythrocyte membrane or cell disease.
enzyme abnormalities that promote irreversible sickling, increase Splenic sequestration is a manifestation of the infarctive process
splenic infarction. The hyposplenism is reversible with transfusion for of sickling in the spleen that extends to involve larger veins.