
Page 1175 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1175
814
PART 6: Neurologic Disorders
20% mannitol 1 g/kg IV bolus ×1 over 15-30 minutes OR 23.4% saline solution 30 mL IVP ×1 over 5 minutes
Check EVD (waveform, level, drainage); drain 3-5 mL of CSF
Level 1: Temporary ICP elevation and crisis
B) Advanced ICP treatment approach
Temporary increase in sedation
Short-term paralysis
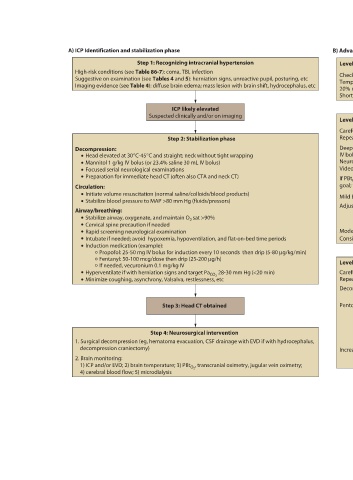
Imaging evidence (see Table 4): diffuse brain edema; mass lesion with brain shift, hydrocephalus, etc
Suggestive on examination (see Tables 4 and 5): herniation signs, unreactive pupil, posturing, etc
Step 1: Recognizing intracranial hypertension
ICP likely elevated Suspected clinically and/or on imaging Level 2: Recurrent or persistent ICP elevation Carefully reassess the patient as in Step 1 Repeat head CT Step 2: Stabilization phase Deepen sedation; switch to midazolam 0.02-0.2 mg/kg/h IV bolus of 20% mannitol 1 g/kg × 1 then 0.5 g/kg × 4-6 h; adjust serum osmolality to target 320-340 mOsm/L Head elevated at 30°C-45°C and straight; neck without tight wrapping Neuromuscular paralysis vecuronium 0.8-1.4 g/kg/min IV infusion rate Mannitol 1 g/kg IV bolus (or 23.4% saline 30 mL IV bolus) Video EEG to exclude non-convulsive seizures Preparation
High-risk conditions (see Table 86-7): coma, TBI, infection
A) ICP Identification and stabilization phase
Decompression: Focused serial neurological examinations Circulation: Airway/breathing: Cervical spine precaution if needed Rapid screening neurological examination Induction medication (example): If needed, vecuronium 0.1 mg/kg IV decompression craniectomy) 2. Brain monitoring: 4) cerebral blood flow; 5) microdialysis
section06.indd 814 1/23/2015 12:56:10 PM