
Page 1400 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1400
CHAPTER 100: Acid-Base Balance 973
the classic distal RTA is a hyperkalemic form, which is actually more increases in cations (rare). Metabolic alkaloses can be divided into those
common than the classic type. The central defect here appears to be in which Cl losses are temporary and can be effectively replaced (chlo-
−
impaired Na transport in the cortical collecting duct. These patients ride responsive) and those in which hormonal mechanisms produce
+
also respond to NaHCO replacement. Proximal (type II) RTA is ongoing losses that can, at best, be offset temporarily by Cl admin-
−
3
characterized by both Na and K reabsorption defects. The disorder istration (chloride resistant) (Fig. 100-2). Similar to hyperchloremic
+
+
is uncommon and usually part of the Fanconi syndrome, where reab- acidosis, these disorders can be distinguished by examination of the
sorption of glucose, phosphate, urate, and amino acids is also impaired. urine [Cl ]. Although much more investigation has focused on acidosis,
−
Treatment of this disorder with NaHCO is ineffective because increased alkalosis appears to be associated with poor prognosis as well. In a pro-
3
ion delivery merely results in increased excretion. Thiazide diuretics spective study, Anderson and Henrich looked at 409 patients with an
38
have been used to treat this disorder with varying success. arterial pH of greater than 7.48. Of these patients, 213 were medical and
Type IV RTA is caused by aldosterone deficiency or resistance. This 196 were surgical. Overall, hospital mortality was 27.9% and increased
disorder is diagnosed by the high serum K and low urine pH (<5.5). as pH values rose, reaching 48.5% when the pH was greater than 7.60.
+
Treatment is usually most effective if the cause can be removed. The While only 2% had pure metabolic alkalosis, patients at greatest risk
most common causes are drugs such as nonsteroidal anti-inflammatory were those with a mixed respiratory and metabolic alkalosis, having a
agents, heparin, or potassium-sparing diuretics. Occasionally, mineralo- mortality of 44.2%.
corticoid replacement is required.
■ GASTROINTESTINAL ACIDOSIS CHLORIDE-RESPONSIvE DISORDERS
Fluid secreted into the gut lumen contains higher amounts of Na than These disorders usually occur as a result of Cl losses from the stomach,
+
−
Cl , similar to the differences in plasma. Extremely large losses of these such as from vomiting or gastric drainage. The treatment involves
−
fluids, particularly if volume is replaced with fluids containing equal lowering the SID, by giving NaCl (since serum [Cl ] will rise greater
−
amounts of Na and Cl , will result in a decrease in the plasma [Na ] than serum [Na ]), KCl, or even HCl (which is most potent because it
+
−
+
+
relative to [Cl ] and a decrease in the SID. contains only strong anions). Saline plus KCl is usually the treatment of
−
■ IATROGENIC ACIDOSIS choice because volume depletion usually coexists with these disorders.
Volume depletion, in turn, stimulates aldosterone secretion, which
+
−
Two of the most common causes of a hyperchloremic metabolic acidosis results in Na reabsorption and the loss of K and Cl .
+
are iatrogenic, and both are due to administration of chloride. Modern Diuretics and other forms of volume contraction produce meta-
parenteral nutrition formulas contain weak anions such as acetate in addi- bolic alkalosis predominantly by stimulating aldosterone, as discussed
tion to Cl , and the balance of each anion can be adjusted depending on earlier. However, diuretics also induce K and Cl excretion directly,
−
+
−
the acid-base status of the patient. If sufficient amounts of weak anions further complicating the problem and inducing metabolic alkalosis
are not provided, the plasma [Cl ] will increase, decreasing the SID and more rapidly.
−
resulting in acidosis. As already discussed, administration of normal
saline can cause a decrease in the SID and, subsequently, an acidosis. CHLORIDE-RESISTANT DISORDERS
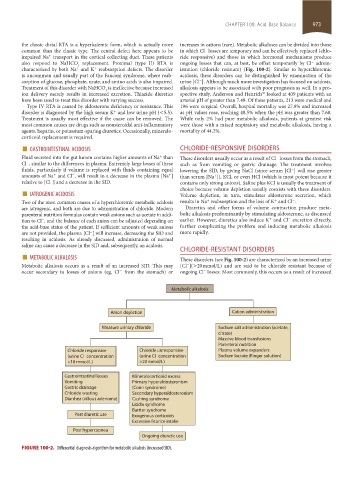
■ METABOLIC ALKALOSIS These disorders (see Fig. 100-2) are characterized by an increased urine
Metabolic alkalosis occurs as a result of an increased SID. This may [Cl ](>20 mmol/L) and are said to be chloride resistant because of
−
occur secondary to losses of anions (eg, Cl from the stomach) or ongoing Cl losses. Most commonly, this occurs as a result of increased
−
−
Metabolic alkalosis
Anion depletion Cation administration
Measure urinary chloride Sodium salt administration (acetate,
citrate)
Massive blood transfusions
Parenteral nutrition
Chloride responsive Chloride unresponsive Plasma volume expanders
–
–
(urine CI concentration (urine CI concentration Sodium lactate (Ringer solution)
<10 mmol/L) >20 mmol/L)
Gastrointestinal losses Mineralocorticoid excess
Vomiting Primary hyperaldosteronism
Gastric drainage (Conn syndrome)
Chloride wasting Secondary hyperaldosteronism
Diarrhea (villous adenoma) Cushing syndrome
Liddle syndrome
Bartter syndrome
Post diuretic use Exogenous corticoids
Excessive licorice intake
Post hypercapnea
Ongoing diuretic use
FIGURE 100-2. Differential diagnosis algorithm for metabolic alkalosis (increased SID).
section08.indd 973 1/14/2015 8:28:27 AM