
Page 1823 - Hall et al (2015) Principles of Critical Care-McGraw-Hill
P. 1823
1292 PART 11: Special Problems in Critical Care
middle and older age groups. Table 129-11 outlines the histopathology
and immunofluorescence findings.
Before the advent of corticosteroids, PV carried a high mortality
rate. At present, patients are typically started on doses of at least 1 to
2 mg/kg per day of prednisone to halt progression of the disease.
Azathioprine may be started concurrently at a dose of 50 to 100 mg/day.
The dose is calculated based on the red blood cell concentration of
thiopurine methyltransferase, an enzyme involved in the metabolism
of the thiopurine drugs. Low concentrations of this enzyme may lead
to serious side effects, such as excessive myelosuppression, whereas
high concentrations may lead to rapid metabolism of azathioprine and
potential underdosing. Immunosuppressants should be initiated early
71
in the course of the disease to allow time for their immunosuppressant
actions to take effect which may take up to 6 weeks. Current thera-
peutic regimens also include parenteral gold, dapsone, plasmapher-
esis, intravenous immune globulin, and other immunosuppressant
agents, such as cyclosporine, cyclophosphamide, and mycophenolate
mofetil. 72,73
■ BULLOUS PEMPHIGOID
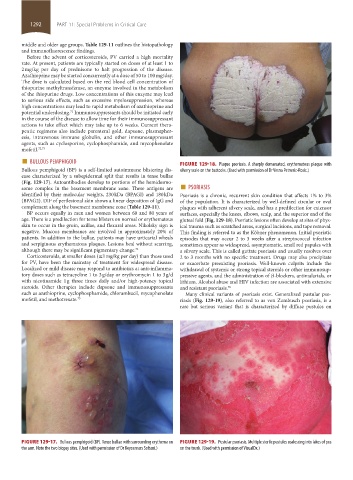
Bullous pemphigoid (BP) is a self-limited autoimmune blistering dis- FIGURE 129-18. Plaque psoriasis. A sharply demarcated, erythematous plaque with
silvery scale on the buttocks. (Used with permission of Dr Vesna Petronic-Rosic.)
ease characterized by a subepidermal split that results in tense bullae
some complex in the basement membrane zone. These antigens are ■ PSORIASIS
(Fig. 129-17). Autoantibodies develop to portions of the hemidesmo-
identified by their molecular weights, 230 kDa (BPAGI) and 180 kDa Psoriasis is a chronic, recurrent skin condition that affects 1% to 3%
(BPAG2). DIF of perilesional skin shows a linear deposition of IgG and of the population. It is characterized by well-defined circular or oval
complement along the basement membrane zone (Table 129-11). plaques with adherent silvery scale, and has a predilection for extensor
BP occurs equally in men and women between 60 and 80 years of surfaces, especially the knees, elbows, scalp, and the superior end of the
age. There is a predilection for tense blisters on normal or erythematous gluteal fold (Fig. 129-18). Psoriatic lesions often develop at sites of phys-
skin to occur in the groin, axillae, and flexural areas. Nikolsky sign is ical trauma such as scratched areas, surgical incisions, and tape removal.
negative. Mucous membranes are involved in approximately 20% of This finding is referred to as the Köbner phenomenon. Initial psoriatic
patients. In addition to the bullae, patients may have urticarial wheals episodes that may occur 2 to 3 weeks after a streptococcal infection
and serpiginous erythematous plaques. Lesions heal without scarring, sometimes appear as widespread, asymptomatic, small red papules with
although there may be significant pigmentary change. 74 a silvery scale. This is called guttate psoriasis and usually resolves over
Corticosteroids, at smaller doses (≤1 mg/kg per day) than those used 2 to 3 months with no specific treatment. Drugs may also precipitate
for PV, have been the mainstay of treatment for widespread disease. or exacerbate preexisting psoriasis. Well-known culprits include the
Localized or mild disease may respond to antibiotics at anti-inflamma- withdrawal of systemic or strong topical steroids or other immunosup-
tory doses such as tetracycline 1 to 3 g/day or erythromycin 1 to 3 g/d pressive agents, and the administration of β-blockers, antimalarials, or
with nicotinamide 1 g three times daily and/or high-potency topical lithium. Alcohol abuse and HIV infection are associated with extensive
steroids. Other therapies include dapsone and immunosuppressants and resistant psoriasis. 76
such as azathioprine, cyclophosphamide, chlorambucil, mycophenolate Many clinical variants of psoriasis exist. Generalized pustular pso-
mofetil, and methotrexate. 75 riasis (Fig. 129-19), also referred to as von Zumbusch psoriasis, is a
rare but serious variant that is characterized by diffuse pustules on
FIGURE 129-17. Bullous pemphigoid (BP). Tense bullae with surrounding erythema on FIGURE 129-19. Pustular psoriasis. Multiple sterile pustules coalescing into lakes of pus
the arm. Note the two biopsy sites. (Used with permission of Dr Keyoumars Soltani.) on the trunk. (Used with permission of VisualDx.)
section11.indd 1292 1/19/2015 10:54:12 AM