
Page 613 - Clinical Hematology_ Theory _ Procedures ( PDFDrive )
P. 613
CHAPTER 29 ■ Body Fluid Analysis 597
Diaphragm
Aorta
Superior recess
Porta hepatis of lesser sac
Lesser omentum
Celiac artery
Pancreas
Lesser sac
Stomach
Superior mesenteric artery
Transverse mesocolon
Third part of duodenum
Transverse colon
Mesentery
Umbilicus
Greater sac
Jejunum
Inferior recess of lesser
sac
Greater omentum
Rectum
Rectouterine pouch
Median umbilical ligament
Uterus
Bladder
Anal canal
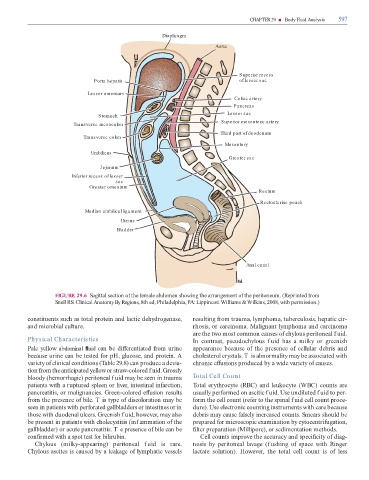
FIGURE 29.6 Sagittal section o the emale abdomen showing the arrangement o the peritoneum. (Reprinted rom
Snell RS. Clinical Anatomy By Regions, 8th ed, Philadelphia, PA: Lippincott Williams & Wilkins, 2008, with permission.)
constituents such as total protein and lactic dehydrogenase, resulting rom trauma, lymphoma, tuberculosis, hepatic cir-
and microbial culture. rhosis, or carcinoma. Malignant lymphoma and carcinoma
are the two most common causes o chylous peritoneal f uid.
Physical Characteristics In contrast, pseudochylous f uid has a milky or greenish
Pale yellow abdominal uid can be di erentiated rom urine appearance because o the presence o cellular debris and
because urine can be tested or pH, glucose, and protein. A cholesterol crystals. T is abnormality may be associated with
variety o clinical conditions ( able 29.8) can produce a devia- chronic e usions produced by a wide variety o causes.
tion rom the anticipated yellow or straw-colored f uid. Grossly
bloody (hemorrhagic) peritoneal f uid may be seen in trauma Total Cell Count
patients with a ruptured spleen or liver, intestinal in arction, otal erythrocyte (RBC) and leukocyte (WBC) counts are
pancreatitis, or malignancies. Green-colored e usion results usually per ormed on ascitic f uid. Use undiluted f uid to per-
rom the presence o bile. T is type o discoloration may be orm the cell count (re er to the spinal f uid cell count proce-
seen in patients with per orated gallbladders or intestines or in dure). Use electronic counting instruments with care because
those with duodenal ulcers. Greenish f uid, however, may also debris may cause alsely increased counts. Smears should be
be present in patients with cholecystitis (inf ammation o the prepared or microscopic examination by cytocentri ugation,
gallbladder) or acute pancreatitis. T e presence o bile can be lter preparation (Millipore), or sedimentation methods.
con rmed with a spot test or bilirubin. Cell counts improve the accuracy and speci city o diag-
Chylous (milky-appearing) peritoneal f uid is rare. nosis by peritoneal lavage (f ushing o space with Ringer
Chylous ascites is caused by a leakage o lymphatic vessels lactate solution). However, the total cell count is o less